Резюме
Актуальність. Використання високої грудної епідуральної блокади (ВГЕБ) при кардіохірургічних операціях може стримуватись побоюванням її негативних гемодинамічних ефектів. Мета. Оцінити вплив ВГЕБ на гемодинаміку при операціях аортокоронарного шунтування (АКШ) зі штучним кровообігом (ШК). Методи. У 85 пацієнтів під час АКШ із ШК визначали серцевий індекс (СІ), ударний індекс, фракцію викиду (ФВ) й індекс загального периферічного судинного опору (ІЗПСО). Результати. Після індукції встановлювався гіподинамічний тип кровообігу: СІ — 2,27 ± 0,69 л • хв–1 • м–2, ІЗПСО — 2618 (2064; 3032) дин • с • см–5 • м–2, при цьому систолічна функція покращувалась, про що свідчило зростання ФВ. Після ШК встановився гіпердинамічний тип кровообігу: СІ зростав до 3,72 ± 0,96 л • хв–1 • м–2 за рахунок ЧСС і систолічної функції серця, а ІЗПСО знижувався. Висновки. При проведенні ВГЕБ під час операцій аортокоронарного шунтування з ШК більшість гемодинамічних параметрів зберігалась у межах референтних значень, а після індукції показники глобальної систолічної функції міокарда зростали, що свідчило про покращення умов роботи серця.
Актуальность. Использование высокой грудной эпидуральной блокады (ВГЭБ) при кардиохирургических операциях может сдерживаться опасением ее негативных гемодинамических эффектов. Цель. Оценить влияние ВГЭБ на гемодинамику при операциях аортокоронарного шунтирования (АКШ) с искусственным кровообращением (ИК). Методы. У 85 пациентов во время АКШ с ИК определяли параметры гемодинамики, включая сердечный индекс (СИ), ударный индекс, фракцию выброса (ФВ) и индекс общего периферического сосудистого сопротивления (ИОПСС). Результаты. После индукции устанавливался гиподинамический тип кровообращения: СИ — 2,27 ± 0,69 л • мин–1 • м–2, ИОПСС — 2618 (2064; 3032) дин • с • см–5 • м–2, при этом систолическая функция улучшалась, о чем свидетельствовал рост ФВ. После ИК установился гипердинамический тип кровообращения: СИ возрастал до 3,72 ± 0,96 л • мин–1 • м–2 за счет частоты сердечных сокращений и систолической функции сердца, а ИОПСС снижался. Выводы. При проведении ВГЕБ во время операций аортокоронарного шунтирования с ИК гемодинамика сохранялась в пределах референтных значений, а после индукции показатели глобальной систолической функции миокарда возрастали, что свидетельствовало об улучшении условий работы сердца.
Objective. The use of high thoracic epidural blockade anesthesia in cardiac operations may be limited due to its adverse hemodynamic effects. Aim. To evaluate the impact of high thoracic epidural blockade anesthesia on hemodynamic during on-bypass coronary artery bypass grafting (CABG). Methods. In 85 patients underwent on-bypass CABG hemodynamic parameters were measured including cardiac index (CI), stroke index (SI), ejection fraction (EF) and systemic vascular resistance index (SVRI). Results. Moderate hypodynamic circulation developed after induction: CI —
2.27 ± 0.69 L • min–1• m–2 and SVRI — 2618 (2064; 3032) din • sec • cm–5 • m–2. Nevertheless systolic function was improving as evidenced by the EF growth. After cardiopulmonary bypass hemodynamic pattern changed over to moderate hyperdynamic one: CI increased to 3.72 ± 0.96 L • min–1 • m–2 due to rise heart rate and improving global systolic cardiac function though SVRI decreased. Conclusion. During on-bypass high thoracic epidural blockade anesthesia majority of hemodynamic parameters kept within reference values. After induction global systolic function grew, indicating an improvement of the heart conditions under the influence of high thoracic epidural blockade anesthesia.
Ключевые слова
висока грудна епідуральна блокада, гемодинаміка, аортокоронарне шунтування, штучний кровообіг.
высокая грудная эпидуральная блокада, гемодинамика, аортокоронарное шунтирование, искусственное кровообращение.
high thoracic epidural blockade, hemodynamics, on-bypass, coronary artery bypass grafting.
Objective. In cardiac surgery have become generally accepted methods «fast-track anesthesia», aimed at reducing of duration and cost of treatment. One of them is high thoracic epidural anesthesia (HTEA). It has some advantages; however, it has not gained popularity in Ukraine. A limiting factor may be fear of negative hemodynamic effects of HTEA in patients with heart disease.
Aim of the work. Evaluate the impact of HTEA on hemodynamic during on-bypass coronary artery bypass grafting (CABG).
Material and methods. The analysis of hemodynamics in 85 patients with coronary heart disease underwent on-bypass CABG who consented to participate in the study according to the form approved by the local ethics committee.
Epidural space was catheterized at the level T5 — T6 and catheter tip was placed at the level T2 — T4. Anesthesia started with bolus 5-6 ml of 0.5% bupivacaine without "adjunct», maintenance — with 0.25 % bupivacaine 6 — 8 ml per hour. General anesthesia included thiopental sodium, diazepam, sodium hydroxybutyrate, guided by BIS index 40 — 60. Before intubation 0.05 mg of fentanyl was used and added as much before incision. Cardiopulmonary bypass (CPB) was conducted at perfusion index 2.4 L•min-1•m-2, moderate hypothermia (core temperature 32 — 34 ○C) and Ht 20 — 25%. The time interval between epidural catheter placement and heparin injection was more than 1 hour.
Before surgery and at arrival to the operating room, induction of anesthesia, sternotomy, after CPB and at the end of the surgery HR (HR), mean arterial pressure (MAP) and central venous pressure (CVP) were recorded. End-diastolic index (EDI), end-systolic index (ESI), stroke and cardiac index (SI, CI), ejection fraction (EF), index of systemic vascular resistance (ISVR) were obtained after induction, sternotomy, termination of CPB and at the end of the surgery with intraoperative transoesophageal ultrasound. Statistics was performed using StatSoft´s «Statistica" v6. Type of distribution was analyzed with Shapiro–Wilk test. Comparison of the data obtained on the contiguous stages of the surgery was performed with Student's t — test at normal and Wilcoxon signed-rank test at asymmetric distribution. Level of statistical significance which allowed to reject the null hypothesis of no difference between the stages was p < 0,05. The data were expressed as mean and standard deviation (M ± s) in normal distribution, and as median and upper and lower quartile (Me (25;75) in asymmetric.
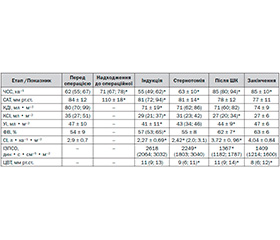
Results. Before surgery the patients had normodynamic circulation, their global systolic function was not impaired. Upon arrival in the operating room HR was 14% higher compared to the preoperative level (p <0.01) and MAP exceeded preoperative level by almost a third (p <0.01). Induction of anesthesia resulted in decrease MAP by 26% and HR — by 23%. EDI, ESI and SI also decreased (p <0.01 for all). In parallel, EF rose (p <0.05). By lowering HR and SI hypodynamic circulation was settled: CI was 2,27 ± 0,69 L•min-1•m-2. After sternotomy a slight but statistically significant increase in HR by 6% was observed (p <0.01); CI increased to 2.42 (2.0; 3.1) L•min-1•m-2 (p <0.05). After termination of CPB marked hemodynamic rearrangement occurred and hyperdynamic pattern of circulation was formed: HR increased by 37%, CI — by half, and ISVR decreased by 39% (p <0.01 for all). At the end of the operation further increase of CI took place. Unlike the two previous stages it was solely on the basis of rise of SI, but the last stage lacked statistical significance. The data are summarized in the table.
Hemodynamics on the stages of the operation under HTEA
|
Етап
Показник
|
Before
surgery
|
Arrival to
operative room
|
Induction
|
Sternotomy
|
After
CPB
|
End
surgery
|
|
HR, min-1
|
62 (55; 67)
|
71 (67; 78) ⃰
|
55 (49; 62) ⃰
|
63 ± 10 ⃰
|
85 (80; 94) ⃰
|
85 ± 10 ⃰
|
|
MAP,
mm Hg
|
84 ± 12
|
110 ± 18 ⃰
|
81 (72; 94) ⃰
|
81 ± 14 ⃰
|
78 ± 12
|
77 ± 11
|
|
EDІ, ml·m-2
|
80 (70; 99)
|
-
|
71 ± 19 ⃰
|
71 (62; 86)
|
71 (60; 82)
|
74 ± 9
|
|
ESI, ml·m-2
|
35 (27; 51)
|
-
|
29 (21; 37) ⃰
|
31 (23; 42)
|
27 (20; 34) ⃰
|
27 ± 6
|
|
SІ, ml·m-2
|
47 ± 10
|
-
|
41 ± 11 ⃰
|
43 (34; 46)
|
44 ± 9 ⃰
|
47 ± 6
|
|
EF, %
|
54 ± 9
|
-
|
57 (53; 65) ⃰
|
55 ± 8
|
62 ± 7 ⃰
|
63 ± 6
|
|
СІ,
L·min-1·m-2
|
2,9 ± 0,7
|
-
|
2,27 ± 0,69 ⃰
|
2,42 ⃰
(2,0; 3,1)
|
3,72±0, 96 ⃰
|
4,04 ± 0,84
|
|
ІSVR,
din·sec
·cm-5·m-2
|
-
|
-
|
2618
(2064;3032)
|
2249 ⃰
(1803;3040)
|
1367 ⃰
(1182;1787)
|
1409
(1214;1600)
|
|
CVP,
mm Hg
|
-
|
-
|
11 (9; 13)
|
9 (6; 11) ⃰
|
11 (9; 14) ⃰
|
8 (6; 12) ⃰
|
⃰ — p < 0,05 comparing with previous stage
Discussion. When arriving at the operating patients had emotional stress, as evidenced by the growth of MAP and HR. Induction led to a pattern of hemodynamics, characterized by moderate hypodynamy. CI reduction primarily resulted from negative chronotropic effect of HTEA and general anesthetics combined with a decrease in blood flow to the heart due to dilation of capacitance vessels. Most of hemodynamic parameters, MAP, CVP, EDI, ESI, SI and EV after induction were within reference values, deviations of CI and ISVR were moderate. It was important that in parallel with a decrease in CI there was a rise of global systolic function, which pointed out to improving of conditions of the heart after HTEA. Median sternotomy is the stage associated with the maximal "surgical stimulation". There were no great fluctuations of hemodynamic parameters at the stage. The increase in HR was explained by compensatory response to relative hypovolemy and gradual restoring of chronotropic properties of the heart. The feature of postbypass period was another rearrangement of hemodynamics and its transition to a hyperdynamic pattern. CI underwent the biggest changes; it grew by 54%, ISVR decreased by 39% (p <0.001 for all). Another feature was that increase of CI resulted from not only rise of HR, but also from improving global systolic function. Data obtained at the end of operations reflect the further trend of improving of hemodynamics, which can be confirmed in larger number of patients.
Conclusion. During on-bypass CABG majority of hemodynamic parameters kept within reference values and did not vary at traumatic stage. Although after induction moderately hypodynamic circulation was set, global systolic function grew, pointing out improvement of the heart condition under the influence of HTEA.
Список литературы
1. Fast-track practice in cardiac surgery: results and predictors of outcome / M. Haanschoten, A. van Straten, J. Woorst et al. // Interact. Cardiovasc. Thorac. Surg. — 2012. — Vol. 15. — P. 989-994. doi: 10.1093/icvts/ivs393.
2. The impact of immediate extubation in the operating room after cardiac surgery onintensive care and hospital lengths of stay / D. Chamchad, J. Horrow, L. Nachamchik et al. // J. Cardiothorac. Vasc. Anesth. — 2010. — Vol. 24. — P. 780-784. doi: 10.1053/j.jvca.2010.04.002.
3. High thoracic epidural analgesia decreases stress hyperglycemia and insulin need in cardiac surgery patients / J. Greisen, D. Nielsen, E. Sloth, C. Jakobsen // Acta Anaesthesiol. Scand. — 2013. — Vol. 57. — P. 171-177. doi: 10.1111/j.1399-6576.2012.02731.x.
4. Effects of high thoracic epidural anesthesia on mixed venous oxy–gen saturation in coronary artery bypass grafting surgery / E. Gurses, D. Berk, H. Sungurtekin // Med. Sci. Monit. — 2013. — Vol. 19. — P. 222-229. doi: 10.12659/MSM.883861.
5. High Thoracic Epidural Analgesia in Cardiac Surgery: Part 1-High Thoracic Epidural Analgesia Improves Cardiac Performance in Cardiac Surgery Patients / C.-J. Jakobsen, R. Bhavsar, D. Nielsen, P. Ryhammer, E. Sloth // Journal of Cardiothoracic and Vascular Anesthesia. — 2012. — Vol. 26. — P. 1039-1047. doi: 10.1053/j.jvca.2012.05.007.
6. Effect of thoracic epidural anasthesia on oxygen delivery and utilization in cardiac surgery patients scheduled to undergor off-pump coronary artery bypass surgery: A prospective study / S. Suryapracash, M. Chakravarthy, A. Gandhi, V. Jawali // Ann. Card. Anaesth. — 2011. — Vol. 14. — P. 192-196. doi: 10.4103/0971-9784.83997.
1. Haanschoten MC, van Straten AH, ter Woorst JF, Stepaniak PS, van der Meer AD, van Zundert AA, Soliman Hamad MA. Fast-track practice in cardiac surgery: results and predictors of outcome. Interact Cardiovasc Thorac Surg. 2012; 15(6):989-94. doi: 10.1093/icvts/ivs393
2. Chamchad D, Horrow JC, Nachamchik L, Sutter FP, Samuels LE, Trace CL, Ferdinand F, Goldman SM. The impact of immediate extubation in the operating room after cardiac surgery on intensive care and hospital lengths of stay.J Cardiothorac Vasc Anesth. 2010; 24:780-784. doi: 10.1053/j.jvca.2010.04.002
3. Greisen J1, Nielsen DV, Sloth E, Jakobsen CJ. High thoracic epidural analgesia decreases stress hyperglycemia and insulin need in cardiac surgery patients. Acta Anaesthesiol Scand. 2013; 57(2):171-7. doi: 10.1111/j.1399-6576.2012.02731.x.
4. Ercan Gurses, Derviş Berk, Hülya Sungurtekin, Asli Mete,and Simay Serin. Effects of high thoracic epidural anesthesia on mixed venous oxygen saturation in coronary artery bypass grafting surgery. Med Sci Monit. 2013; 19:222–229. doi: 10.12659/MSM.883861
5. Jakobsen CJ, Bhavsar R, Nielsen DV, Ryhammer PK, Sloth E, Greisen J. High Thoracic Epidural Analgesia in Cardiac Surgery: Part 1—High Thoracic Epidural Analgesia Improves Cardiac Performance in Cardiac Surgery Patients. Journal of Cardiothoracic and Vascular Anesthesia. 2012; 26:1039-1047. doi: 10.1053/j.jvca.2012.05.007.
6. Suryaprakash S, Chakravarthy M, Gautam M, Gandhi A, Jawali V, Patil T, Jayaprakash K, Pandey S, Muniraju G. Effect of thoracic epidural anasthesia on oxygen delivery and utilization in cardiac surgery patients scheduled to undergor off-pump coronary artery bypass surgery: A prospective study. Ann Card Anaesth. 2011; 14:192 — 196. doi: 10.4103/0971-9784.83997.