
Архив офтальмологии Украины Том 11, №2, 2023
Вернуться к номеру
Епітеліальний профіль рогівки і стабільність рефракції після ексимерлазерної корекції аметропії, виконаної на різних платформах
Авторы: Панченко Ю.О., Путієнко О.О., Косуба С.І.
Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
Рубрики: Офтальмология
Разделы: Клинические исследования
Версия для печати
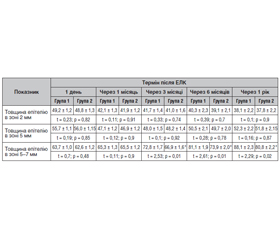
Актуальність. За даними 2020 року, 161 млн світової популяції мали аметропії, які пов’язані з помірними та тяжкими порушеннями зору або сліпотою. Лазерний кератомільоз in situ (LASIK) широко використовується у світі для корекції міопії, гіперметропії та астигматизму. Гіперметропічний профіль ексимерлазерної абляції призначений для збільшення кривизни центральної ділянки. Лазери попереднього покоління та попередні профілі абляції асоціювалися зі значним регресом, недокорекцією та втратою максимальної скоригованої гостроти зору на відстані. Оцінка профілю епітелію відіграє важливу роль для визначення механізму виникнення і ризиків регресу рефракційного результату. Мета: оцінити епітеліальний профіль рогівки і стабільність рефракції після ексимерлазерної корекції (ЕЛК) аметропії, виконаної на різних платформах. Матеріали та методи. Було проаналізовано медичну документацію 40 пацієнтів (80 очей), віком 18–40 років, яким з 2021 по 2023 р. проводили ЕЛК методом LASIK для корекції гіперметропії у медичному центрі «Лазер плюс» (м. Львів, Україна). До 1-ї групи увійшли 22 пацієнти (44 ока), яким було виконано ЕЛК методом LASIK для корекції гіперметропії за допомогою ексимерного лазера MEL 80 (Carl Zeiss Meditec). Групу 2 становили 18 пацієнтів (36 очей), яким виконували ЕЛК методом LASIK для корекції гіперметропії за допомогою ексимерного лазера MEL 90 (Carl Zeiss Meditec). Динамічні зміни оцінювались за допомогою контролю маніфестної рефракції, а також за картами товщини епітелію за результатами ОСТ рогівки. Термін спостереження — 1 рік. Результати. У групі 1 максимальна товщина епітелію фіксувалась на межі 5- і 7-міліметрової зони, а в групі 2 — на 7 мм. Різке збільшення товщини епітелію в обох групах фіксувалось у термін 3 місяці після LASIK. У 2-й групі найбільший приріст товщини був на 10 % меншим, ніж в 1-й групі. Незначний гіперметропічний зсув на термінах з 3-го місяця до 1 року. Статистично значущої різниці між результатами двох досліджуваних груп на різних термінах післяопераційного спостереження не відмічалось. Висновки. Поточне дослідження при даному об’ємі і тривалості показало, що результуючий профіль товщини епітелію є достатньо стабільним для підтримки необхідної сили заломлення рогівки протягом 1 року спостереження, але потрібний контроль цих параметрів на віддалених термінах, враховуючи різницю приросту товщини епітелію після LASIK на різних ексимерлазерних платформах — MEL 80 і MEL 90.
Background. According to 2020 data, 161 million of the world’s population had ametropia associated with moderate to severe visual impairment or blindness. The laser-assisted in situ keratomileusis (LASIK) is widely used in the world to correct myopia, hypermetropia and astigmatism. The hypermetropic profile of excimer laser ablation is designed to increase the curvature of the central area. Previous generation lasers and previous ablation profiles have been associated with significant regression, undercorrection, and loss of maximum corrected distance visual acuity. Evaluating the profile of the epithelium is important for determining the mechanism of occurrence and risks of regression of the refractive result. The purpose of the study: to evaluate the corneal epithelial profile and refractive stability after excimer laser correction (ELC) for ametropia performed on different platforms. Materials and methods. The medical documentation of 40 patients (80 eyes) aged 18–40 years were analyzed, they underwent ELC by the LASIK to correct hypermetropia at the Laser Plus Medical Center (Lviv, Ukraine) in 2021–2023. The first group included 22 patients (44 eyes) who underwent ELC by the LASIK to correct hypermetropia using the MEL 80 excimer laser (Carl Zeiss Meditec). Group 2 consisted of 18 patients (36 eyes) who underwent ELC by the LASIK to correct hypermetropia using the MEL 90 excimer laser (Carl Zeiss Meditec). Changes were evaluated by monitoring the manifest refraction, as well as by maps of the epithelial thickness based on the results of corneal optical coherence tomography. The observation period was 1 year. Results. In the first group, the maximum epithelial thickness was at the border of 5- and 7-millimeter zone, and in the second group — at 7 mm. The epithelial thickness rapidly increased in both groups on the third month after LASIK. In the second group, the highest increase in epithelial thickness was 10 % less than in the first group. Slight hypermetropic shift was observed in the period from 3 months to 1 year. There was no statistically significant difference between the results of the two studied groups at different periods of postoperative follow-up. Conclusions. The current study at this volume and duration showed that the resulting profile of epithelial thickness is stable enough to maintain the required corneal refractive power during the 1-year follow-up, but long-term monitoring of these parameters is required, given the difference in an increase in the epithelial thickness after LASIK on different excimer laser platforms — MEL 80 and MEL 90.
ексимерлазерна корекція; аметропія; LASIK; епітеліальний профіль рогівки; стабільність рефракції
excimer laser correction; ametropia; LASIK; corneal epithelial profile; refractive stability
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Burton M.J. et al. The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. The Lancet Global Health. Vol. 9, Iss. 4. e489-e551.
- Dausch D., Smecka Z., Klein R., Schroder E., Kirchner S. Excimer laser photorefractive keratectomy for hyperopia. J. Cataract. Refract Surg. 1997. 23. 169-176.
- Barraquer J.I. Queratomileusis y queratofakia. Bogota: Instituto Barraquer de America, 1980. 342.
- Reinstein D.Z., Archer T. Combined Artemis very high-frequency digital ultrasound-assisted transepithelial phototherapeutic keratectomy and wavefront-guided treatment following multiple corneal refractive procedures. J. Cataract. Refract. Surg. 2006. 32. 1870-1876.
- Kermani O., Schmeidt K., Oberheide U., Gerten G. Hyperopic laser in situ keratomileusis with 5.5-, 6.5-, and 7.0-mm optical zones. J. Refract. Surg. 2005. 21. 52-58.
- Kanellopoulos A.J. Topography-guided hyperopic and hyperopic astigmatism femtosecond laser-assisted LASIK: long-term experience with the 400 Hz eye-Q excimer platform. Clin. Ophthalmol. 2012. 6. 895-901.
- de Ortueta D., Arba-Mosquera S. Laser in situ keratomileusis for high hyperopia with corneal vertex centration and asymmetric offset. Eur. J. Ophthalmol. 2016. 27. 141-152.
- Reinstein D.Z., Carp G.I., Archer T.J., et al. LASIK for the correction of high hyperopic astigmatism with epithelial thickness mo–nitoring. J. Refract. Surg. 2017. 33. 314-321.
- Reinstein D.Z., Srivannaboon S., Gobbe M., Archer T.J., Silverman R.H., Sutton H., Coleman D.J. Epithelial thickness profile changes induced by myopic LASIK as measured by Artemis very high- frequency digital ultrasound. J. Refract. Surg. 2009. 25. 444-450.
- Li H., Han Q., Zhang J., Shao T., Wang H., Long K. Role of corneal epithelial thickness during myopic regression in femtosecond laser-assisted in situ keratomileusis and transepithelial photorefractive keratectomy. BMC Ophthalmol. 2022 Dec 8. 22(1). 481. doi: 10.1186/s12886-022-02727-x. PMID: 36482343; PMCID: PMC9733129.
- Chen H., Wang Z., Li K., Wang Y., Li X., Du L., Lin M., Savini G., Wang Q., Yu A., Chen S. Agreement Between Predicted and Actual Measured Ablation Depth After FS-LASIK Using Different Rotating Scheimpflug Cameras and OCT. Front. Med. (Lausanne). 2022 May 19. 9. 907334. doi: 10.3389/fmed.2022.907334. PMID: 35665335; PMCID: PMC9160334.
- Reinstein D.Z., Silverman R.H., Sutton H.F., Coleman D.J. Very high-frequency ultrasound corneal analysis identifies anatomic correlates of optical complications of lamellar refractive surgery: anatomic diagnosis in lamellar surgery. Ophthalmology. 1999. 106. 474-482.
- Lohmann C.P., Güell J.L. Regression after LASIK for the treatment of myopia: the role of the corneal epithelium. Semin. Ophthalmol. 1998. 13. 79-82.
- Erie J.C., Patel S.V., McLaren J.W., Ramirez M., Hodge D.O., Maguire L.J., Bourne W.M. Effect of myopic laser in situ keratomileusis on epithelial and stromal thickness: a confocal microscopy study. Ophthalmology. 2002. 109. 1447-1452.
- Spadea L., Fasciani R., Necozione S., Balestrazzi E. Role of the corneal epithelium in refractive changes following laser in situ keratomileusis for high myopia. J. Refract. Surg. 2000. 16. 133-139.
- Gauthier C.A., Holden B.A., Epstein D., Tengroth B., Fagerholm P., Hamberg-Nyström H. Role of epithelial hyperplasia in regression following photorefractive keratectomy. Br. J. Ophthalmol. 1996. 80. 545-548.
- Reinstein D.Z., Ameline B., Puech M., Montefiore G., Laroche L. VHF digital ultrasound three-dimensional scanning in the diagnosis of myopic regression after corneal refractive surgery. J. Refract. Surg. 2005. 21. 480-484.
- Могілевський С., Жовтоштан М., Бушуєва О.В. Персистуючий синдром сухого ока після ексимерлазерної корекції міопії та віддалені функціональні результати. Офтальмологічний журнал. 2023, лютий. Вип. 1. С. 19-26. doi: 10.31288/oftalmolzh202311926.
- Patel S.V., Erie J.C., McLaren J.W., Bourne W.M. Confocal microscopy changes in epithelial and stromal thickness up to 7 years after LASIK and photorefractive keratectomy for myopia. J. Refract. Surg. 2007. 23. 385-392.
- Scroggs M.W., Proia A.D. Histopathological variation in keratoconus. Cornea. 1992. 11. 553-559.
- Haque S., Simpson T., Jones L. Corneal and epithelial thickness in keratoconus: a comparison of ultrasonic pachymetry, Orbscan II, and optical coherence tomography. J. Refract. Surg. 2006. 22. 486-493.
- Aktekin M., Sargon M.F., Cakar P., Celik H.H., Firat E. Ultrastructure of the cornea epithelium in keratoconus. Okajimas Folia Anat. Jpn. 1998. 75. 45-53.
- Reinstein D.Z., Gobbe M., Archer T.J., Silverman R.H., Coleman D.J. Epithelial, stromal, and total corneal thickness in keratoconus: three-dimensional display with Artemis very high-frequency digital ultrasound. J. Refract. Surg. 2010. 26. 259-271.
- Reinstein D.Z., Archer T.J., Gobbe M. Corneal epithelial thickness profile in the diagnosis of keratoconus. J. Refract. Surg. 2009. 25. 604-610.
- Benlarbi A., Kallel S., David C., Barugel R., Hays Q., Goemaere I., et al. Asymmetric Intrastromal Corneal Ring Segments with Progressive Base Width and Thickness for Keratoconus: Evaluation of Efficacy and Analysis of Epithelial Remodeling. J. Clin. Med. 2023 Feb 20. 12(4). 1673. doi: 10.3390/jcm12041673. PMID: 36836208; PMCID: PMC9962479.
- Varley G.A., Huang D., Rapuano C.J., Schallhorn S., Boxer Wachler B.S., Sugar A.; Ophthalmic Technology Assessment Committee Refractive Surgery Panel, American Academy of Ophthalmology. LASIK for hyperopia, hyperopic astigmatism, and mixed astigmatism: a report by the American Academy of Ophthalmology. Ophthalmology. 2004. 111. 1604-1617.
- Reinstein D.Z., Archer T.J., Gobbe M., Silverman R.H., Coleman D.J. Epithelial thickness after hyperopic LASIK: three-dimensional display with Artemis very high-frequency digital ultrasound. J. Refract. Surg. 2010 Aug. 26(8). 555-64. doi: 10.3928/1081597X-20091105-02. PMID: 19928697; PMCID: PMC4492162.
- Reinstein D.Z., Srivannaboon S., Gobbe M., Archer T.J., Silverman R.H., Sutton H., Coleman D.J. Epithelial thickness profile changes induced by myopic LASIK as measured by Artemis very high- frequency digital ultrasound. J. Refract. Surg. 2009. 25. 444-450.
- de Ortueta D., von Rüden D., Arba-Mosquera S. Refractive Effect of Epithelial Remodelling in Myopia after Transepithelial Photorefractive Keratectomy. Vision (Basel). 2022 Dec 13. 6(4). 74. doi: 10.3390/vision6040074. PMID: 36548936; PMCID: PMC9781313.
- Jaycock P.D., O’Brart D.P., Rajan M.S., Marshall J. 5-year follow-up of LASIK for hyperopia. Ophthalmology. 2005. 112. 191-199.
- Esquenazi S. Five-year follow-up of laser in situ keratomileusis for hyperopia using the Technolas Keracor 117C excimer laser. J. Refract. Surg. 2004. 20. 356-363.
- Desai R.U., Jain A., Manche E.E. Long-term follow-up of hyperopic laser in situ keratomileusis correction using the Star S2 excimer laser. J. Cataract. Refract. Surg. 2008. 34. 232-237.
- Reinstein D.Z., Carp G.I., Archer T.J., Day A.C., Vida R.S. Outcomes for Hyperopic LASIK with the MEL 90® Excimer Laser. J. Refract. Surg. 2018 Dec 1. 34(12). 799-808. doi: 10.3928/1081597X-20181019-01. PMID: 30540362.