
Международный неврологический журнал Том 20, №3, 2024
Вернуться к номеру
Порушення мови: діагностика та лікування у неврологічній практиці
Авторы: Дубенко О.Є. (1), Фломін Ю.В. (2, 3), Защипась Ю.П. (2), Прокопів М.М. (3), Тріщинська М.А. (4), Кавецька В.В. (5), Данько Р.В. (6)
(1) - Харківський національний медичний університет, м. Харків, Україна
(2) - Медичний центр «Універсальна клініка «Оберіг», м. Київ, Україна
(3) - Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
(4) - Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
(5) - Медичний реабілітаційний центр «Модричі», с. Модричі, Львівська обл., Україна
(6) - Черкаський обласний клінічний госпіталь ветеранів війни, м. Черкаси, Україна
Рубрики: Неврология
Разделы: Справочник специалиста
Версия для печати
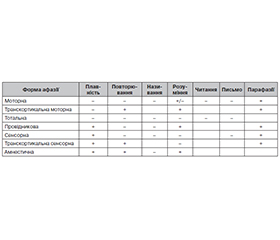
Порушення мовних функцій, що виникають внаслідок мозкового інсульту чи інших вогнищевих уражень головного мозку, а також при деяких нейродегенеративних захворюваннях (афазія), часто зустрічаються у неврологічній практиці і мають негативний вплив на практично всі види соціальної взаємодії та якість життя пацієнтів. Мета роботи полягала у вивченні та узагальненні відомостей світової наукової літератури щодо афазії для досягнення консенсусу серед представників різних спеціальностей та оптимізації тактики лікувально-діагностичних заходів у пацієнтів з порушеннями мови. У PubMed, Clinical Key Elsevier, Cochrane Library та Google Scholar був проведений пошук публікацій за період 2001–2023 рр., що присвячені порушенням мови при неврологічних захворюваннях, діагностиці та лікуванню афазій. У статті висвітлені історичні аспекти формування сучасних уявлень про порушення мови та розглянуті основні клінічні форми афазії, їх зв’язок з топографією уражень головного мозку. Діагностичні підходи при порушеннях мови та мовлення включають оцінювання мовної продукції, розуміння мови, називання предметів, повторення, читання та письма, а також вимови та плавності мови, яке у клінічній практиці виконують лікарі-невропатологи і терапевти мови та мовлення (логопеди). На основі комплексного оцінювання мовних функцій порушення мови можна класифікувати як одну або кілька з семи основних клінічних форм афазії. Головними провісниками кращого відновлення мовних функцій є менша початкова тяжкість афазії, ранній початок лікування та достатній обсяг допомоги. Основою лікування та реабілітації при афазії є терапія мови та мовлення, яку можуть проводити як фахівці, так і родина пацієнта чи доглядальники. Роль медикаментозного лікування та неінвазивної стимуляції мозку у поліпшенні мовних функцій поки є дуже обмеженою і потребує подальших досліджень. Велике значення має навчання пацієнта та його родини певним особливостям комунікації при порушеннях мови. Майбутні стратегії лікування афазії, ймовірно, будуть полягати у комбінації поведінкового підходу з фармакотерапевтичними та нейромодуляційними втручаннями.
Language disorders resulting from cerebral stroke or other focal brain lesions, as well as from some neurodegenerative diseases (aphasia) are common in neurological practice and have a negative impact on almost all kinds of social interaction and the quality of life of patients. The aim of this work was to study and summarize the information on aphasia in the world scientific lite-rature in order to achieve a consensus among representatives of different specialties and to optimize the diagnostic and treatment strategies in patients with language disorders. We searched for publications from 2001 to 2023 on language disorders in neurological diseases, diagnosis, and treatment of aphasia in the PubMed, Clinical Key Elsevier, Cochrane Library, and Google Scholar databases. The article highlights the historical aspects of the formation of modern ideas about language disorders and considers the main clinical forms of aphasia, their relationship with the topography of brain lesions. Diagnostic approaches in speech and language disorders include assessment of speech production, speech comprehension, naming, repetition, reading and writing, in addition to pronunciation and fluency, which is performed in clinical practice by neurologists, speech and language therapists. Based on a comprehensive assessment of language functions, language impairment can be classified as one or more of the seven main clinical forms of aphasia. The main predictors of a better recovery of language functions are a milder initial severity of aphasia, an earlier initiation of treatment and an adequate scope of therapy. The basis of treatment and rehabilitation for aphasia is speech and language therapy, which can be carried out by both specialists and the patient’s family or caregivers. The role of drug treatment and non-invasive brain stimulation in improving language functions is still very limited and requires further research. Teaching patients and their family certain rules of communication taking into account present language disorders is of great importance. Future treatment strategies for aphasia are likely to consist of a combination of a behavioral approach with pharmacotherapeutic and neuromodulatory interventions.
порушення мови; афазія; неврологічна практика; мозковий інсульт; терапія мови та мовлення; діагностика; лікування; реабілітація; огляд
language disorder; aphasia; neurological practice; stroke; speech and language therapy; diagnosis; treatment; rehabilitation; review