
Oral and General Health Том 6, №1, 2025
Вернуться к номеру
Візуалізація скронево-нижньощелепного суглоба в нейром’язовій гнатології
Авторы: Мірза Р.О.
Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
Рубрики: Стоматология
Разделы: Клинические исследования
Версия для печати
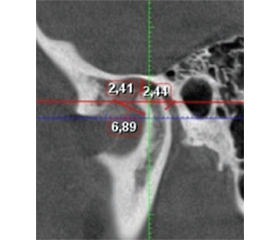
Актуальність. Підвищення ефективності методів визначення співвідношення щелеп для виконання оклюзійної реабілітації є одним з основних завдань функціональної стоматології. Співвідношення щелеп, отримане для здійснення протезування зубних рядів, вважається кінцевим варіантам, а співвідношення щелеп перед тривалою оклюзійною реабілітацією частіше розглядається як попереднє. У зв’язку з цим можуть бути затребуваними різні підходи у лікуванні дисфункції скронево-нижньощелепного суглоба. Мета: визначити ефективність технології лікування дисфункції скронево-нижньощелепного суглоба на підставі аналізу комп’ютерних томограм. Матеріали та методи. Виконувалось клінічне обстеження пацієнтів з ознаками дисфункції скронево-нижньощелепного суглоба, яка визначається за наявністю хрусту, клацання, крепітації в скронево-нижньощелепному суглобі, болю в поверхневих жувальних м’язах при пальпації і шляхом збору анамнезу. Комп’ютерна томографія виконувалась за звичної оклюзії і за співвідношення щелеп, отриманого після депрограмування жувальних м’язів за допомогою нейром’язової електростимуляції. Аналіз гіпсових моделей зубних рядів здійснювався між центральними різцями верхньої і нижньої щелеп. Результати. На підставі аналізу комп’ютерних томограм скронево-нижньощелепного суглоба виявлено, що дистальне положення суглобової головки в суглобовій ямці у 43 обстежених, виражене як співвідношення передньої і задньої суглобових щілин, становило 1 : 0,23–0,85, при цьому за одиницю прийнято розмір передньої суглобової щілини. З’ясовано, що розміри передньої, верхньої, задньої суглобових щілин можуть змінюватись під впливом нейром’язової електростимуляції в межах відповідно 1,32 ± 0,38 мм, 2,14 ± 0,35 мм, 2,12 ± 0,35 мм для правої сторони і 1,42 ± 0,38 мм, 2,12 ± 0,35 мм, 2,19 ± 0,37 мм для лівої сторони (р = 0,05). Висновки. Виявлено ефективність методу фізіотерапевтичного лікування дисфункції скронево-нижньощелепного суглоба на підставі клінічного огляду й аналізу комп’ютерних томограм. Визначено, що значення, за яких може відбуватись зміна положення суглобової головки після депрограмування жувальних м’язів, є оптимальними для лікування дисфункції скронево-нижньощелепних суглобів із застосуванням гнатологічних шин.
Background. Enhancing the accuracy of jaw relationship assessment for occlusal rehabilitation remains a fundamental objective in functional dentistry. The mandibular position established for prosthetic restoration is considered definitive, whereas the jaw relationship before extended occlusal rehabilitation is often regarded as provisional. As a result, different approaches to managing temporomandibular joint (TMJ) dysfunction may be warranted. Evaluating the effectiveness of treatment methods for temporomandibular joint dysfunction through the analysis of computed tomography scans remains a relevant and important issue. Materials and methods. A clinical assessment was conducted on patients presenting with TMJ dysfunction symptoms, including clicking, popping, crepitus, and tenderness in the superficial masticatory muscles upon palpation. Patient history was also taken into account. Computed tomography (CT) scans were performed in habitual occlusion and in a jaw position obtained following masticatory muscle deprogramming using neuromuscular electrical stimulation. Additionally, analysis of dental arch models was conducted by assessing the position of the upper and lower central incisors. Results. CT analysis of the TMJ in 43 patients revealed a distal condylar position within the glenoid fossa. The ratio of the anterior to posterior joint spaces was 1 : 0.23–0.85, with the anterior joint space used as the reference unit. It was found that the dimensions of the anterior, superior, and posterior joint spaces varied following neuromuscular electrical stimulation: for right TMJ — accordingly, 1.32 ± 0.38 mm, 2.14 ± 0.35 mm, 2.12 ± 0.35 mm, for left TMJ — 1.42 ± 0.38 mm, 2.12 ± 0.35 mm, 2.19 ± 0.37 mm (р = 0.05). Conclusions. Clinical evaluation and CT analysis confirmed the efficacy of a physiotherapeutic approach in treating TMJ dysfunction. The observed changes in condylar positioning following masticatory muscle deprogramming suggest that neuromuscular treatment protocols, including gnathological splints, may provide an optimal therapeutic outcome for managing TMJ dysfunction.
комп’ютерна томографія; скронево-нижньощелепний суглоб; нейром’язова електростимуляція
computer tomography; temporomandibular joint; neuromuscular electrical stimulation