
Журнал «Медицина неотложных состояний» Том 21, №5, 2025
Вернуться к номеру
Динаміка поліморфноядерних нейтрофільних лейкоцитів як критерій ефективності лікування спонтанного бактеріального перитоніту
Авторы: Беседінський М.С., Тутченко М.І.
Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
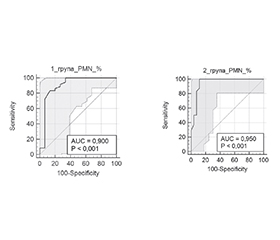
Актуальність. Спонтанний бактеріальний перитоніт (СБП) є тяжким ускладненням декомпенсованого цирозу печінки (ЦП) з асцитом та асоціюється з високим ризиком летальності. Незважаючи на сучасні підходи в лікуванні, ефективність емпіричної антибіотикотерапії значно варіює, особливо при нозокоміальних формах СБП, що часто спричинені мультирезистентною флорою. Рання діагностика СБП та контроль ефективності лікування потребують виконання рутинного парацентезу з підрахунком поліморфноядерних нейтрофілів (PMN). Однак оптимальні порогові значення зниження PMN та їх прогностична цінність при різних формах СБП залишаються недостатньо вивченими. Мета: проаналізувати динаміку PMN в асцитичній рідині через 48 годин як показник ефективності емпіричної антибіотикотерапії при СБП у пацієнтів з ЦП та порівняти динаміку PMN при позагоспітальній та нозокоміальній формах СБП. Матеріали та методи. У це дослідження включено пацієнтів з ЦП та підтвердженим СБП (n = 101), госпіталізованих до КНП «Київська міська клінічна лікарня швидкої медичної допомоги» у 2023–2025 рр. Пацієнтів розподілено на дві групи залежно від форми СБП: позагоспітальна (n = 51) та нозокоміальна (n = 50). Діагностика здійснювалася шляхом виконання діагностичного парацентезу з підрахунком PMN (≥ 250 кл/мм3) та бактеріологічним аналізом асцитичної рідини. Через 48 год усім пацієнтам виконували повторний парацентез із підрахунком PMN для оцінки динаміки. Аналіз виконано з використанням програм Statistica v10, MedCalc 23.2.1 та Microsoft Excel. Для кількісних змінних обчислювали середнє стандартне відхилення та/або медіану з міжквартильним інтервалом (Me, IQR). Для міжгрупових порівнянь використовували t-тест Стьюдента або U-критерій Манна — Уїтні. Частотні характеристики аналізували за -критерієм Пірсона. Прогностичну цінність динаміки PMN оцінювали за допомогою ROC-аналізу з розрахунком AUC, 95% CI, оптимального порогу (Youden index), чутливості та специфічності. Результати. У 31,7 % пацієнтів перебіг СБП мав безсимптомний характер або клінічна симптоматика була неспецифічною, що ускладнювало діагностику. Це обґрунтовує необхідність рутинного парацентезу всім пацієнтам з клінічно значущим асцитом. Первинна антибіотикотерапія була ефективною загалом у 67,3 % випадків, причому в позагоспітальній групі позитивна відповідь на лікування спостерігалась у 70,5 % пацієнтів порівняно з нозокоміальною — 48 %. Динаміка нейтрофільозу вірогідно відрізнялася між групами: середній відсоток зниження PMN через 48 годин був вищим при позагоспітальному СБП порівняно з нозокоміальним. Проведений ROC-аналіз демонструє, що для позагоспітального СБП найкращим прогностичним порогом було зниження PMN на 36,8 %, тоді як для нозокоміального — > 16 %. Висновки. Рутинне виконання діагностичного парацентезу, а також його повторне виконання через 48 годин є доцільним незалежно від наявності симптомів СБП. Динаміка рівня PMN в асцитичній рідині після 48 годин антибіотикотерапії є надійним індикатором відповіді на лікування. Отримані результати вказують на доцільність використання різних порогів зниження PMN залежно від форми СБП. Госпітальний СБП характеризується менш вираженою відповіддю на стартову терапію, що обґрунтовує необхідність первинного призначення антибіотиків з урахуванням поширеності резистентної мікрофлори.
Background. Spontaneous bacterial peritonitis (SBP) is a life-threatening complication of decompensated liver cirrhosis (LC) with ascites and is associated with high mortality. Despite modern treatment approaches, the efficacy of empirical antibiotic therapy remains variable, particularly in nosocomial SBP, which is frequently caused by multidrug-resistant organisms. Early diagnosis and evaluation of treatment efficacy require routine paracentesis with polymorphonuclear neutrophil (PMN) count. However, the optimal PMN reduction thresholds and their prognostic significance across different SBP forms remain poorly defined. Objective: to evaluate PMN dynamics in ascitic fluid after 48 hours as a marker of response to empirical antibiotic treatment in patients with SBP and LC, and to compare this indicator between community-acquired and nosocomial SBP. Materials and methods. A prospective cohort study was conducted in 101 patients with LC and confirmed SBP, hospitalized at the Kyiv City Clinical Emergency Hospital from 2023 to 2025. They were divided into two groups: community-acquired (n = 51) and nosocomial SBP (n = 50). Diagnostic paracentesis was performed with PMN count (≥ 250 cells/mm3) and microbiological culture of ascitic fluid. Follow-up paracentesis was done after 48 hours to assess PMN dynamics. Statistical analysis was performed using Statistica v10, MedCalc v23.2.1, and Microsoft Excel. For quantitative variables, mean ± standard deviation and/or median with interquartile range were calculated. Intergroup comparisons were conducted using Student’s t-test or the Mann-Whitney U test. Categorical variables were analyzed with Pearson’s test. The prognostic value of PMN dynamics was assessed by receiver operating characteristic (ROC) analysis, with calculation of area under the ROC curve, 95% confidence intervals, Youden index, sensitivity and specificity. Results. In 31.7 % of patients, SBP was asymptomatic or presented with nonspecific symptoms, complicating diagnosis. This underscores the importance of routine paracentesis in all patients with clinically significant ascites. Overall, empirical antibiotic therapy was effective in 67.3 % of cases, with better outcomes in the community-acquired group (70.5 %) compared to the nosocomial group (48 %). Neutrophil dynamics differed significantly between groups: the average PMN reduction after 48 hours was higher in community-acquired SBP. ROC analysis showed optimal thresholds of > 36.8 % PMN reduction for community-acquired SBP and > 16 % for nosocomial SBP. Conclusions. Routine diagnostic paracentesis on admission and repeated after 48 hours should be performed regardless of SBP symptoms. PMN dynamics in the ascitic fluid after 48 hours of antibiotic therapy is a reliable marker of treatment efficacy. The findings support using different PMN thresholds depending on SBP form. Nosocomial SBP is associated with reduced treatment response, warranting broader-spectrum antibiotics from the outset, taking into account the prevalence of resistant microflora.
цироз печінки; портальна гіпертензія; асцит; спонтанний бактеріальний перитоніт; нейтрофільоз; парацентез
liver cirrhosis; portal hypertension; ascites; spontaneous bacterial peritonitis; neutrophilosis; paracentesis
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Biggins SW, Angeli P, Garcia-Tsao G, Gins P, Ling SC,
- Nadim MK, et al. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome: 2021 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2021;74(2):1014-1048. doi: 10.1002/hep.31884.
- Hadjivasilis A, Agrawal A. The diagnostic accuracy of ascitic calprotectin for the early diagnosis of spontaneous bacterial peritonitis: Systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2021; 33(3):312-318. doi: 10.1097/MEG.0000000000001813.
- Na SH, Kim EJ, Nam EY, Song KH, Choe PG, Park WB, et al. Comparison of clinical characteristics and outcomes of spontaneous bacterial peritonitis and culture negative neutrocytic ascites. Scand J Gastroenterol. 2017;52(2):199-203. doi: 10.1080/00365521.2016.1245776.
- Lutz P, Nischalke HD, Krmer B, Goeser F, Kaczmarek DJ, Schlabe S, et al. Antibiotic resistance in healthcare-related and nosocomial spontaneous bacterial peritonitis. Eur J Clin Invest. 2017;47(1):44-52. doi: 10.1111/eci.12701.
- Niu B, Kim B, Limketkai BN, Sun J, Li Z, Woreta T, Chen PH. Mortality from spontaneous bacterial peritonitis among hospitalized patients in the USA. Dig Dis Sci. 2018;63(5):1327-1333. doi: 10.1007/s10620-018-4970-9.
- Hung TH, Lee HF, Wang CY, Tsai CC. Short and long-term mortality of spontaneous bacterial peritonitis in cirrhotic patients: a nationwide population-based study. BMC Gastroenterol. 2024;24(1):45. doi: 10.1186/s12876-024-02789-6.
- Kolosovych IV, Hanol IV, Lebedieva KO. Features of perfor–ming abdominal paracentesis in complicated course of acute pancreatitis. Odes Med J. 2023;2(183):56-60. doi: 10.32782/2226-2008-2023-2-10.
- Kim JJ, Tsukamoto MM, Mathur AK, Ghomri YM, Hou LA, Sheibani S, Runyon BA. Delayed paracentesis is associated with increased in-hospital mortality in patients with spontaneous bacterial peritonitis. Am J Gastroenterol. 2014 Sep;109(9):1436-42. doi: 10.1038/ajg.2014.212.
- Lal Krishna U, Deni J, Ramu M, Sandesh K, Saji K Sebastian, Gaurav Khatana, Gino R Philip. Spontaneous Bacterial Peritonitis: Etiology, Microbiology, and Clinical Outcomes in Cirrhosis Patients. Cureus. 2024 Dec 31;16(12):e76679. doi: 10.7759/cureus.76679.
- Serper M, Pulaski M, Zhang S, Taddei T, Kaplan D, Mahmud N. Albumin for Spontaneous Bacterial Peritonitis: Care Variation, Disparities, and Outcomes. The American Journal of Gastroenterology 2024 Nov 12:10.14309/ajg.0000000000003190. doi: 10.14309/ajg.0000000000003190
- Tay PWL, Xiao J, Tan DJH, Ng C, Lye YN, Lim WH, et al. An Epidemiological Meta-Analysis on the Worldwide Prevalence, Resistance, and Outcomes of Spontaneous Bacterial Peritonitis in Cirrhosis. Front Med (Lausanne). 2021 Aug 5;8:693652. doi: 10.3389/fmed.2021.693652.
- Shi L, Wu D, Wei L, et al. Nosocomial and Community-Acquired Spontaneous Bacterial Peritonitis in patients with liver cirrhosis in China: Comparative Microbiology and Therapeutic Implications. Sci Rep 7, 46025(2017). https://doi.org/10.1038/srep46025.
- Iqbal A, Gangwani MK, Beran A, Dahiya DS, Sohail AH, Lee-Smith W, et al. Nosocomial vs healthcare associated vs community acquired spontaneous bacterial peritonitis: Network meta-analysis. Am J Med Sci. 2023 Oct;366(4):305-313. doi: 10.1016/j.amjms.2023.06.014.
- Piano S, Fasolato S, Salinas F, Romano A, Tonon M, Morando F, et al. The empirical antibiotic treatment of nosocomial spontaneous bacterial peritonitis: Results of a randomized, controlled clinical trial. Hepatology. 2016 Apr;63(4):1299-309. doi: 10.1002/hep.27941.
- European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. 2018 Oct. Available from: https://easl.eu/wp-content/uploads/2018/10/decompensated-cirrhosis-English-report.pdf.
- Hasan I, Nababan SHH, Handayu AD, Aprilicia G, Gani RA. Scoring system for predicting 90-day mortality of in-hospital liver cirrhosis patients at Cipto Mangunkusumo Hospital. BMC Gastroenterol. 2023 Jun 1;23(1):190. doi: 10.1186/s12876-023-02813-4.
- Tutchenko M, Rudyk D, Besedinskyi M, Chub S. Spontaneous bacterial peritonitis. Eastern Ukrainian Medical Journal. 2024;12(2):221-228. https://doi.org/10.21272/eumj.2024;12(2):221-228
- Tutchenko M, Besedinskyi M, Aslanian S, Kluzko I, Rudyk D, Chub S. Hepatorenal syndrome in decompensated portal hypertension. Medicni Perspektivi. 2024;29(4):94-101. https://doi.org/10.26641/2307-0404.2024.4.319225
- Saffo S, To UK, Santoiemma PP, Laurito M, Haque L, Rabiee A, et al. Changes in Ascitic Fluid Polymorphonuclear Cell Count After Antibiotics Are Associated With Mortality in Spontaneous Bacterial Peritonitis. Clin Gastroenterol Hepatol. 2022 May;20(5):e1201-e1204. doi: 10.1016/j.cgh.2021.07.019.
- Samonakis DN, Gatselis N, Bellou A, Sifaki-Pistolla D, Mela M, Demetriou G, et al. Spontaneous bacterial peritonitis: a prospective Greek multicenter study of its epidemiology, microbiology, and outcomes. Ann Gastroenterol. 2022 Jan-Feb;35(1):80-87. doi: 10.20524/aog.2021.0674.