
Журнал «Медицина неотложных состояний» Том 21, №5, 2025
Вернуться к номеру
Результати хірургічного лікування переломів дистального епіметафіза великогомілкової кістки: ретроспективний аналіз
Авторы: Бур’янов О.А., Цапенко Г.С., Омельченко Т.М.
Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
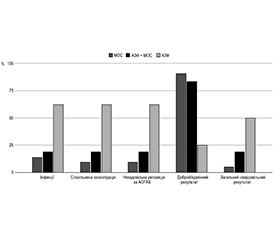
Актуальність. Переломи дистального епіметафіза великогомілкової кістки (пілонні переломи) є складними внутрішньосуглобовими ушкодженнями. Їх лікування пов’язане зі значними труднощами, високим ризиком ускладнень (інфекції, незрощення, посттравматичний артроз) та часто незадовільними функціональними результатами, незважаючи на сучасні хірургічні підходи. Залишається актуальним пошук оптимальної тактики лікування. Мета: ретроспективно оцінити результати різних методів хірургічного лікування переломів дистального епіметафіза великогомілкової кістки у 67 пацієнтів, пролікованих у спеціалізованому центрі політравми, та проаналізувати фактори, що асоціюються з незадовільними результатами лікування. Матеріали та методи. Проведено ретроспективний аналіз 67 пацієнтів (вік 18–60 років) з пілонними переломами, пролікованих у 2015–2024 рр. Порівнювали групи: одноетапний металоостеосинтез (МОС, n = 22), двохетапне лікування (апарат зовнішньої фіксації (АЗФ) з подальшим МОС, n = 37) та остаточна фіксація в АЗФ (n = 8). Оцінювали частоту ускладнень (інфекції, незрощення, сповільнена консолідація), якість репозиції суглобової поверхні, функціональний результат за шкалою American Orthopaedic Foot and Ankle Society (AOFAS) через 12 місяців. Незадовільний результат визначався як необхідність виконання артродезу або ампутації, розвиток глибокої інфекції або показник за шкалою AOFAS < 70 балів. Статистичний аналіз проводили за допомогою точного критерію Фішера (p < 0,05). Результати. У досліджуваній когорті частота зрощення переломів становила 94,0 %, тоді як незрощення діагностовано у 6,0 % випадків. Глибокі інфекційні ускладнення виникли у 9,0 % пацієнтів. Рятівні операції, як-от вторинний артродез або ампутація, не виконувались (0 %). Відмінний або добрий функціональний результат (AOFAS ≥ 80 балів) через 12 місяців після операції був досягнутий у 79,1 % пацієнтів. Незадовільний функціональний результат (AOFAS < 70 балів) спостерігався у 7,5 % (n = 5) пацієнтів, причому всі ці випадки були асоційовані з переломами типу С за класифікацією АО/ОТА (p = 0,008). При порівнянні методів лікування остаточна фіксація в АЗФ асоціювалася зі статистично значущо вищою частотою поверхневих інфекцій (p = 0,039), будь-яких інфекційних ускладнень (p = 0,020), сповільненої консолідації (p = 0,012) та незадовільної якості репозиції (p = 0,004). Також у цій групі відзначалася нижча частка пацієнтів з результатом AOFAS ≥ 80 балів (p = 0,002) та вища загальна частота незадовільних результатів лікування (p = 0,022) порівняно з групами одноетапного МОС та двохетапного лікування (АЗФ + МОС). Результати одноетапного МОС та двохетапного лікування були переважно порівнянними, за винятком дещо вищої частоти сповільненої консолідації при двохетапному підході. Висновки. Лікування пілонних переломів залишається складним завданням, особливо при ушкодженнях типу С. У цій когорті пацієнтів застосування внутрішнього остеосинтезу, як одноетапного, так і двохетапного, продемонструвало суттєві переваги над остаточною фіксацією в апараті зовнішньої фіксації за основними показниками результатів лікування.
Background. Distal epimetaphyseal fractures of the tibia (pilon fractures) are complex intra-articular injuries. Their treatment is associated with significant difficulties, a high risk of complications (infection, nonunion, post-traumatic arthritis), and often unsatisfactory functional outcomes despite modern surgical approaches. The optimal surgical strategy remains debated. The objective of this study was to retrospectively evaluate the outcomes of different surgical treatments for distal epimetaphyseal fractures of the tibia in 67 patients treated at a specialized polytrauma center and to analyze factors associated with unsatisfactory treatment results. Materials and methods. We performed a retrospective analysis of 67 patients (aged 18–60) treated for pilon fractures between 2015 and 2024. We compared groups based on the method used: single-stage open reduction and internal fixation (ORIF, n = 22), two-stage treatment (external fixation (ExFx) followed by ORIF, n = 37), and definitive external fixation (n = 8). We assessed outcomes including complication rates (infection, nonunion, delayed union), quality of articular reduction, and functional outcome using the American Orthopaedic Foot and Ankle Society (AOFAS) score at 12 months. An unsatisfactory outcome was defined as the need for arthrodesis or amputation, development of deep infection, or an AOFAS score < 70. Fisher’s exact test was used for statistical analysis (p < 0.05). Results. In the studied cohort, the union rate was 94.0 %, while nonunion was diagnosed in 6.0 % of cases. Deep infectious complications occurred in 9.0 % of patients. Salvage procedures, such as secondary arthrodesis or amputation, were not performed (0 %). An excellent or good functional outcome (AOFAS ≥ 80 points) at 12 months post-surgery was achieved in 79.1 % of patients. An unsatisfactory functional outcome (AOFAS < 70 points) was observed in 7.5 % (n = 5) of patients, with all these cases being associated with AO/OTA type C fractures (p = 0.008). When comparing treatment methods, definitive external fixation was associated with significantly higher rates of superficial infections (p = 0.039), any infectious complications (p = 0.020), delayed union (p = 0.012), and poor quality of reduction (p = 0.004). This group also had a lower proportion of patients with an AOFAS score ≥ 80 points (p = 0.002), and a higher overall rate of unsatisfactory treatment outcomes (p = 0.022) compared to the groups of single-stage ORIF and two-stage treatment (ExFx + ORIF). The results of single-stage ORIF and two-stage treatment were mostly comparable, except for a slightly higher rate of delayed union with the two-stage approach. Conclusions. The treatment of pilon fractures remains a challenging task, especially for type C injuries. In this patient cohort, the use of internal fixation, both single- or two-stage, demonstrated significant advantages over definitive external fixation in terms of key treatment outcome indicators.
переломи пілона; дистальний відділ великогомілкової кістки; внутрішній остеосинтез; зовнішня фіксація; результати лікування; ускладнення
pilon fractures; distal tibia; internal fixation; external fixation; treatment outcomes; complications
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Mauffrey C, Vasario G, Battiston B, Lewis C, Beazley J, Seligson D. Tibial pilon fractures: a review of incidence, diagnosis, treatment, and complications. Acta Orthop Belg. 2011 Aug;77(4):432-40. PMID: 21954749.
- Mandi DM, Belin RP, Banks J, Barrett B. Pilon fractures. Clin Podiatr Med Surg. 2012 Apr;29(2):243-78, viii. doi: 10.1016/j.cpm.2012.01.001.
- Bourne RB. Pylon fractures of the distal tibia. Clin Orthop Relat Res. 1989 Mar;(240):42-6. PMID: 2917444.
- Kelikian H, Kelikian AS. Disorders of the ankle. Philadelphia (PA): WB Saunders Co; 1985.
- Mandracchia VJ, Evans RD, Nelson SC, Smith KM. Pilon fractures of the distal tibia. Clin Podiatr Med Surg. 1999 Oct;16(4):743-67. PMID: 10553230.
- Meng YC, Zhou XH. External fixation versus open reduction and internal fixation for tibial pilon fractures: A meta-analysis based on observational studies. Chin J Traumatol. 2016 Oct 1;19(5):278-82. doi: 10.1016/j.cjtee.2016.06.002.
- Marsh JL, Slongo TF, Agel J, Broderick JS, Jakobsson B, Kregor PJ, et al. Fracture and dislocation classification compendium: Orthopaedic Trauma Association Classification, Database and Outcomes Committee. J Orthop Trauma. 2007;21(10 Suppl):S1-133. doi: 10.1097/00005131-200711101-00001.
- Koulouvaris P, Stafylas K, Mitsionis G, Vekris M, Mavrodontidis A, Xenakis T. Long-term results of various therapy concepts in severe pilon fractures. Arch Orthop Trauma Surg. 2007 Jul;127(5):313-20. doi: 10.1007/s00402-007-0306-y.
- Oken OF, Yildirim AO, Asilturk M. Finite element analysis of the stability of AO/OTA 43-C1 type distal tibial fractures treated with distal tibia medial anatomic plate versus anterolateral anatomic plate. Acta Orthop Traumatol Turc. 2017 Oct;51(5):404-8. doi: 10.1016/j.aott.2017.09.003.
- Tang X, Liu L, Tu CQ, Li J, Li Q, Pei FX. Comparison of early and delayed open reduction and internal fixation for treating closed tibial pilon fractures. Foot Ankle Int. 2014 Jul;35(7):657-64. doi: 10.1177/1071100714534214.
- Zheng Y, Zhang JD, Shen JM, Chen JJ, Toy L, Huang JF. A modified 2-stage treatment for AO/OTA 43-C1 pilon fractures accompanied by distal fibular and posterior lip of the distal tibia fracture. J Foot Ankle Surg. 2020 Sep-Oct;59(5):972-8. doi: 10.1053/j.jfas.2020.03.020.
- Carbonell-Escobar R, Rubio-Suarez JC, Ibarzabal-Gil A, Rodriguez-Merchan EC. Analysis of the variables affecting outcome in fractures of the tibial pilon treated by open reduction and internal fixation. J Clin Orthop Trauma. 2017 Oct-Dec;8(4):332-8. doi: 10.1016/j.jcot.2017.05.014.
- McFerran MA, Smith SW, Boulas HJ, Schwartz HS. Complications encountered in the treatment of pilon fractures. J Orthop Trauma. 1992 Jun;6(2):195-200. doi: 10.1097/00005131-199206000-00011.
- Ruedi TP, Allgower M. Fractures of the lower end of the tibia into the ankle joint. Injury. 1969;1(2):92-9. doi: 10.1016/s0020-1383(69)80053-1.
- Borrelli J Jr, Ellis E. Pilon fractures: assessment and treatment. Orthop Clin North Am. 2002 Jan;33(1):231-45, x. doi: 10.1016/s0030-5898(03)00082-8.
- Topliss CJ, Jackson M, Atkins RM. Anatomy of pilon fractures of the distal tibia. J Bone Joint Surg Br. 2005 May;87(5):692-7. doi: 10.1302/0301-620X.87B5.15761.
- R Core Team. R: A language and environment for statistical computing. Vienna (Austria). R Foundation for Statistical Computing. 2024 May 28. Available from: https://www.R-project.org/.
- Flores M, Ciminero M, Kottmeier SA, Botros D, Zelle BA, Shearer DW. Pilon fractures: Consensus and controversy. OTA Int. 2023;6(3 Suppl):e236. doi: 10.1097/OI9.0000000000000236.
- van der Vliet QMJ, Ochen Y, McTague MF, Weaver MJ, Hietbrink F, Houwert RM, et al. Long-term outcomes after operative treatment for tibial pilon fractures. OTA Int. 2019 Nov 22;2(4):e043. doi: 10.1097/OI9.0000000000000043.
- Erichsen JL, Andersen PI, Viberg B, Jensen C, Damborg F, Froberg L. A systematic review and meta-analysis of functional outcomes and complications following external fixation or open reduction internal fixation for distal intra-articular tibial fractures: an update. Eur J Orthop Surg Traumatol. 2019 May;29(4):907-17. doi: 10.1007/s00590-019-02368-9.
- Sourougeon Y, Barzilai Y, Haba Y, Spector B, Prat D, Eilig D, et al. Outcomes following minimally invasive plate osteosynthesis (MIPO) application in tibial pilon fractures — a systematic review. Foot Ankle Surg. 2023 Dec;29(8):566-75. doi: 10.1016/j.fas.2023.07.013.
- Michelitsch C, Stillhard PF, Sommer C. Pilonfrakturen: Therapiegrundstze und chirurgische Strategie. Unfallchirurgie (Heidelb). 2025 Feb;128(2):117-29. German. doi: 10.1007/s00113-024-01511-4.
- Gao Y, Zhao Y, Wang H, Xu X, Cheng Z, Lu T, et al. Three-dimensional heat map: the OTA/AO type 43C pilon fracture lines distribution. Int J Gen Med. 2024 Jan 30;17:323-34. doi: 10.2147/IJGM.S444977.
- Perugini A, Hyland S, Iandoli J, Hill Z, Peabody J, DeGenova D, et al. The impact of fibular fixation method on pilon fracture healing. J Clin Med. 2025 Jan 9;14(2):358. doi: 10.3390/jcm14020358.
- Salama AM, El-Desouky MA, Al-Shenqiti AM, Alnaeem H, Attia M, Abdelmonem M. Comparison of temporary external fixation and open reduction with internal fixation for the management of pilon fractures: a short-term outcome prospective clinical trial. Cureus. 2024 May 7;16(5):e60003. doi: 10.7759/cureus.60003.
- Jain N, Saini UC, Bali K, Sandhu KS, Dhillon MS, Devgan A. Functional outcomes of pilon fractures treated by external fixation, delayed plating, and open reduction and internal fixation (ORIF): a prospective cohort study. Cureus. 2024 Nov 30;16(11):e74867. doi: 10.7759/cureus.74867.
- Liu G, Li Z, Li L, Chen W, Liu J, Chen X, et al. Treatment of AO/OTA type 43-C3 pilon fractures with a combination of miniplate and main plate: a retrospective analysis. BMC Musculoskelet Disord. 2025 Apr 28;26(1):368. doi: 10.1186/s12891-025-08280-x.