
Журнал "Гастроэнтерология" Том 59, №3, 2025
Вернуться к номеру
Грижа стравохідного отвору діафрагми, ахалазія стравоходу: якість життя і тригерні фактори розвитку в умовах війни
Авторы: Бабій О.М., Демешкіна Л.В., Шевченко Б.Ф., Пролом Н.В., Зеленюк О.В.
ДУ «Інститут гастроентерології НАМН України», м. Дніпро, Україна
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
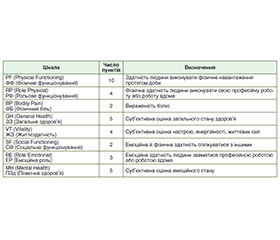
Актуальність. Стравохідно-шлунковий перехід має складний анатомо-функціональний механізм, неспроможність якого супроводжується розвитком грижі стравохідного отвору діафрагми (ГСОД) або ахалазії стравоходу (АС), що потребує хірургічної корекції. На сьогодні, в умовах війни, оцінка якості життя (ЯЖ) і визначення тригерних факторів, що сприяють розвитку ГСОД і АС, є актуальними питаннями гастроентерології. Мета: дослідити ЯЖ і тригерні фактори, які могли сприяти розвитку ГСОД та АС в умовах війни, за даними анкетування. Матеріали та методи. У відділенні хірургії органів травлення обстежено 90 хворих за період із січня 2023 року по грудень 2024 року, серед них 66 пацієнтів з діагнозом ГСОД і 24 хворих з діагнозом АС. Контрольну групу становили 20 здорових осіб. Серед обстежених хворих з ГСОД (n = 66) було 49 (74,2 %) чоловіків і 17 (25,8 %) жінок. Серед обстежених хворих з АС (n = 24) було 17 (70,8 %) чоловіків і 7 (29,2 %) жінок. Середній вік усіх хворих становив (47,13 ± 2,81) року. Частину хворих становили військовослужбовці — 39 (43,3 %). Для оцінки ЯЖ використовували загальний опитувальник SF-36. Для оцінки впливу можливих тригерних факторів на розвиток ГСОД та АС нами було розроблено опитувальник з урахуванням впливу війни. Результати. Встановлено, що ЯЖ значно знижена (р < 0,05) у хворих з ГСОД та АС незалежно від статусу (військовослужбовець або пересічний громадянин). За оцінкою ЯЖ досліджених пацієнтів встановлено, що показники фізичного та психічного компонентів здоров’я були нижчими за показники контрольної групи в 1,6 (р < 0,05) раза в обох групах, при ГСОД показник фізичного компонента здоров’я був в 1,4 (р < 0,05) раза нижче, ніж при АС, а показник психічного компонента здоров’я був в 1,7 (р < 0,05) раза нижче при АС, ніж при ГСОД. При анкетуванні пацієнтами визначено можливі тригерні фактори: тривале й незвичне тяжке фізичне навантаження (59,1 %) — для розвитку ГСОД (χ2 = 15,27; р < 0,001) і тривалий незвичний стрес-фактор (45,8 % ) — для розвитку АС (χ2 = 41,04; р = 0,044). Висновки. За оцінкою ЯЖ досліджених пацієнтів в умовах війни встановлено, що показник фізичного компонента здоров’я був нижче при ГСОД, ніж при АС, а показник психічного компонента здоров’я був нижче при АС, ніж при ГСОД. Визначено, що в умовах війни тригерним фактором, що сприяв розвитку ГСОД, було тривале й незвичне тяжке фізичне навантаження, а розвитку АС міг сприяти тривалий незвичний стрес-фактор.
Background. The esophagogastric junction has a complex anatomical and functional mechanism whose failure is accompanied by the development of hiatal hernia (HН) or esophageal achalasia (EA) requiring surgical correction. Today, in wartime conditions, assessing the quality of life (QOL) and identifying factors contributing to the development of HН and EA are relevant issues in gastroenterology. The aim of the study: to investigate QOL and the impact of trigger factors on the development of HH and EA in war conditions based on questionnaire data. Materials and methods. In the digestive system surgery department, 90 patients were examined between January 2023 and December 2024, of whom 66 were diagnosed with HH and 24 had EA. The control group consisted of 20 healthy individuals. Among the examined patients with HH, there were 49 (74.2 %) men and 17 (25.8 %) women. EA group included 17 (70.8 %) men and 7 (29.2 %) women. The average patients’ age was (47.13 ± 2.81) years. Thirty-nine (43.3 %) patients were military. The general SF-36 questionnaire was used to assess QOL. To study the impact of possible trigger factors on the development of HH and EA, we developed a questionnaire taking into account war factors. Results. It was found that QOL is significantly reduced (p < 0.05) in patients with HH and EA, regardless of status (military serviceman or ordinary citizen). Assessment of QOL in the examined patients revealed that the indicators of physical and mental components were lower than those in controls, by 1.6 (p < 0.05) times for both groups. In HH, the indicator of the physical component of health was 1.4 (p < 0.05) times lower than in EA, and the indicator of the mental component of health was 1.7 (p < 0.05) times lower in EA than in HH. When questioned, patients identified possible trigger factors: prolonged and unusually heavy physical exertion (59.1 %) for the development of HH (χ2 = 15.27; p < 0.001) and prolonged stress factor (45.8 %) for the possible development of EA (χ2 = 41.04; p = 0.044). Conclusions. According to the assessment of the QOL in the examined patients during wartime conditions, it was found that the indicator of physical health component was lower in HH than in EA, and the indicator of mental health component was lower in EA than in HH. It was determined that in wartime conditions, the trigger factors contributing to the development of HH were prolonged and unusually heavy physical exertion, and EA might be provoked by an unusual, prolonged stress factor.
ахалазія стравоходу; грижа стравохідного отвору діафрагми; якість життя; тригерні фактори; в умовах війни
esophageal achalasia; hiatal hernia; quality of life; trigger factors; war conditions
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Pomenti S, Blackett JW, Jodorkovsky D. Achalasia: Diagnosis, Management and Surveillance. Gastroenterol Clin North Am. 2021;50(4):721-736. doi: 10.1016/j.gtc.2021.07.001.
- Aiolfi A, Bonavina L. Hot topics in Hiatal Hernia. Hernia. 2024;28(5):1495-1496. doi: 10.1007/s10029-024-03176-9.
- Marvel S, Monnet E. Laparoscopic Treatment of Sliding Hiatal Hernia. Vet Clin North Am Small Anim Pract. 2024;54(4):649-659. doi: 10.1016/j.cvsm.2024.02.009.
- Mari A, Abu Baker F, Pellicano R, Khoury T. Diagnosis and Management of Achalasia: Updates of the Last Two Years. J Clin Med. 2021;10(16):3607. doi: 10.3390/jcm10163607.
- Yu HX, Han CS, Xue JR, Han ZF, Xin H. Esophageal hiatal hernia: risk, diagnosis and management. Expert Rev Gastroenterol Hepatol. 2018;12(4):319-329. doi: 10.1080/17474124.2018.1441711.
- Kim P, Turcotte J, Park A. Hiatal hernia classification — Way past its shelf life. Surgery. 2021;170(2):642-643. doi: 10.1016/j.surg.2021.02.062.
- Provenza CG, Romanelli JR. Achalasia: Diagnosis and Mana–gement. Surg Clin North Am. 2025;105(1):143-158. doi: 10.1016/j.suc.2024.06.011.
- Momodu II, Wallen JM. Achalasia. 2023. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. PMID: 30137800.
- Rengarajan A, Bazarbashi AN, Gyawali CP. Pathophysiology of achalasia. Digestion. 2025;10:1-17. doi: 10.1159/000547354.
- Hiatal hernia. https://sokl.com.ua/grizha-stravoxidnogo-otvoru-diafragmi. Accessed: August 22, 2025 (in Ukrainian).
- Alsahafi MA, Alajhar NA, Almahyawi AO, Alsulami HH, Alghamdi WA, Alharbi LA, et al. The prevalence and risk factors for hiatal hernia among patients undergoing endoscopy: A retrospective analysis. Saudi Med J. 2023;44(5):509-512. doi: 10.15537/smj.2023.44.5.20220903.
- Musbahi A, Mahawar K. Hiatal hernia. Br J Surg. 2023;110(4):401-402. doi: 10.1093/bjs/znac449.
- Dunn CP, Patel TA, Bildzukewicz NA, Henning JR, Lipham JC. Which hiatal hernia’s need to be fixed? Large, small or none? Ann Laparosc Endosc Surg. 2020;5:29 doi: 10.21037/ales.2020.04.02.
- Kiosov OM. New approaches in the treatment of achalasia cardia and development of methods for relapse prevention. Future of science: innovations and perspectives. Proceedings of II International Scientific and Practical Conference Stockholm, Sweden. 23–25 December. 2024:77-79.
- Torres-Aguilera M, Remes Troche JM. Achalasia and esophageal cancer: risks and links. Clin Exp Gastroenterol. 2018;11:309-316. doi: 10.2147/CEG.S141642.
- Lee K, Hong SP, Yoo IK, Yeniova AÖ, Hahn JW, et al. Global trends in incidence and prevalence of achalasia, 1925–2021: A systematic review and meta-analysis. United European Gastroenterol J. 2024;12(4):504-515. doi: 10.1002/ueg2.12555.
- Kharroubi SA, Elbarazi I. Editorial: Health-related quality of life in health care. Front Public Health. 2023;11:1123180. doi: 10.3389/fpubh.2023.1123180.
- Peláez Mata DJ, Del Valle Gómez P, de Agustín Asensio JC. Quality of life in adolescents who underwent congenital diaphragmatic hernia surgical repair. Cir Pediatr. 2022;35(3):118-124. doi: 10.54847/cp.2022.03.14.
- Kvitka DM, Palamarchuk VO, Zemskov SV, Sichinava RM. Introducing of quality of life into practical medicine. Clinical Endocrinology and Endocrine Surgery. 2021;1:70-75. doi: 10.30978/CEES-2021-1-70 (in Ukrainian).
- Teoli D, Bhardwaj A. Quality Of Life. 2023. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. PMID: 30725647.
- Haraldstad K, Wahl A, Andenæs R. et al. LIVSFORSK network. A systematic review of quality of life research in medicine and health sciences. Qual Life Res. 2019;28(10):2641-2650. doi: 10.1007/s11136-019-02214-9.
- Measuring Quality of Life. https://www.who.int/tools/whoqol/whoqol-100. Accessed: August 27, 2025.
- Kivelä AJ, Kauppi J, Räsänen J, But A, Sintonen H, et al. Long-Term Health-Related Quality of Life (HRQoL) After Redo-Fundoplication. World J Surg. 2021;45(5):1495-1502. doi: 10.1007/s00268-021-05954-3.
- Kharroubi SA, Elbarazi I. Editorial: Health-related quality of life in health care. Front Public Health. 2023;11:1123180. doi: 10.3389/fpubh.2023.1123180.
- Palenzuela D, Paudel M, Petrusa E, Maltby A, Andrus S, Paranjape C. Patients report significant improvement in quality of life following hiatal hernia repair-despite recurrence. Surg Endosc. 2024;38(10):6001-6007. doi: 10.1007/s00464-024-11106-0.
- Ware JE Jr. SF-36 health survey update. Spine (Phila Pa 1976). 2000;25(24):3130-3139. doi: 10.1097/00007632-200012150-00008.
- Wang S, Barrett E, Hicks MH, et al. Associations between mental health symptoms, trauma, quality of life and coping in adults living in Ukraine: A cross-sectional study a year after the 2022 Russian invasion. Psychiatry Res. 2024;339:116056. doi: 10.1016/j.psychres.2024.116056.
- Lebid I.G. The predictive significance of physical and mental components of health related quality of life questionnaire SF-36 in adults with congenital heart disease. Ukrainian J of Cardiovascular Surgery. 2018;1(30):44-48 (in Ukrainian).
- Makarova OP, Chervonyi PD. The essence of stress and its effect on the human body in extreme conditions. Social Psychology. Legal Psychology. 2023;46:222-226. https://doi.org/10.32782/2663-5208.2023.46.36 (in Ukrainian).
- Kucher S, Vorontsova T, Smachilo I, Vereshchagina N, Ganberger I, Horishniy I. Assessment of quality of life using the SF-36 questionnaire: Analysis of literary data Journal “Perspectives and Innovations of Science” (Series “Pedagogy”, Series “Psychology”, Series “Medicine:). 2024;4(38):1313-1324. DOI: https://doi.org/10.52058/2786-4952-2024-4(38)-1313-1324 (in Ukrainian).
- Shastry N, Sultana E, Jeffrey M, Collado F, Kibler J, DeLucia C, et al. The impact of post-traumatic stress on quality of life and fatigue in women with Gulf War Illness. BMC Psychol. 2022;10(1):42. doi: 10.1186/s40359-022-00752-5.
- Gifford EJ, Boyle SH, Vahey J, Sims KJ, Efird JT, Chesnut B, et al. Health-Related Quality of Life by Gulf War Illness Case Status. Int J Environ Res Public Health. 2022;19(8):4425. doi: 10.3390/ijerph19084425.
- Dubenko A, Morelli R, Cross JH, Hall J, Kharytonov V, Michaelis R, Wiebe S; ILAE Emergency Task Force for Ukraine. Mental health and quality of life of individuals with epilepsy during the war in Ukraine. Epilepsia. 2024;65(9):2718-2727. doi: 10.1111/epi.18052.
- Buchcik J, Kovach V, Adedeji A. Mental health outcomes and quality of life of Ukrainian refugees in Germany. Health Qual Life Outcomes. 2023;21(1):23. doi: 10.1186/s12955-023-02101-5.