
Журнал "Гастроэнтерология" Том 59, №3, 2025
Вернуться к номеру
Особливості раку шлунка в Іраку
Авторы: Israa S. Abdulameer (1), Ahmed Alshewered (2), Anwar Sheikha (2)
(1) - Oncology and Nuclear Medicine Center, Al-Imam Al-Sadiq Teaching Hospital, Babylon Health Directorate, Ministry of Health, Babylon, Iraq
(2) - Misan Radiation Oncology Center, Misan Health Directorate, Ministry of Health, Misan, Iraq
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
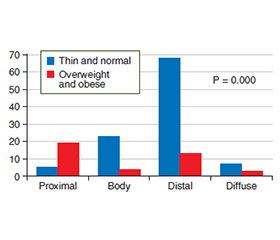
Актуальність. Рак шлунка є четвертим за поширеністю типом раку у світі. У цьому дослідженні зроблено спробу торкнутися цієї важливої проблеми та з’ясувати її стан в Іраку, зважаючи на відносно несприятливий прогноз захворювання та низьку відповідь на лікування. Мета: визначити особливості перебігу раку шлунка та фактори ризику в іракській популяції. Матеріали та методи. Серед доступних регіонів із надійним збором даних ми обрали два (Сулейманія з відомим онкологічним центром Хіва та Вавилон) для всебічного вивчення демографії, клінічних проявів, поширеності, типу пухлини, локалізації та стадії захворювання, індексу маси тіла й несприятливого анамнезу хвороби. Також враховували соціально-економічний статус і рівень освіти. Критично аналізували тип харчування, вживання солоної, гострої їжі й температуру страв. Фіксували дані щодо групи крові, сімейного анамнезу, статусу куріння та вживання алкоголю. Результати. У дослідження залучено 150 пацієнтів із раком шлунка. Співвідношення чоловіків та жінок дорівнювало 1,3 : 1. Медіана віку пацієнтів чоловічої та жіночої статі становила відповідно 61 та 52 роки. Розподіл пухлин за анатомічною локалізацією наступний: дистальний відділ — 83 (55 %) пацієнти, проксимальний — 26 (17 %), тіло та дно шлунка — 16 (11 %), ураження всього шлунка — 12 (8 %). У 13 (9 %) випадках пухлина була в ділянці малої кривизни. Найпоширенішим гістологічним підтипом є аденокарцинома кишкового типу — 69 пацієнтів (46 %). Дифузний тип виявлено в 43 (29 %) осіб, у 14 (9 %) — змішаний, а у 24 (16 %) гістопатологічні зміні були некласифіковані. Виразкову форму діагностовано в 57 % випадків, поліпоподібні або грибоподібні ураження — у 28 %, інфільтративні — у 15 %. Найпоширенішою ендоскопічною знахідкою є виразковий тип (57 % пацієнтів). У більшості випадків рак шлунка (44 %) був IV стадії. Серед осіб із IV стадією лише 11 мали статус Her-2: негативний — у 10 випадках (15,15 %) та позитивний — в одному. Найчастішим місцем метастазування була печінка, далі — очеревина. Висновки. Попри низьку поширеність, деякі епідеміологічні характеристики раку шлунка в Іраку нагадують такі в країнах високого ризику. Найбільша кількість випадків раку шлунка припадає на аденокарциному. Більшості пацієнтів 40–60 років. Захворюваність на рак шлунка в осіб молодше 50 років вища, ніж у західному світі. Порівняно із західною літературою пацієнти в Іраку частіше мали аденокарциному кишкового типу та рідше — дифузний тип. У більшості випадків зафіксовано пізні стадії захворювання.
Background. Gastric cancer is the fourth most common cancer in the world. In this research project, we tried to touch this important topic and find out where we stand in regard to this cancer with its relatively poor prognosis and lack of response to treatment. The study aimed to determine the gastric cancer pattern, and risk factors in Iraqi population. Materials and methods. Of the approachable regions with trustable data collection, we chose two regions: Sulaymaniyah and its renowned Hiwa Cancer Center and Babylon to comprehensively study demography, clinical presentations, prevalence, tumor type, site and stage of the disease, body mass index and adverse past medical history. Socioeconomic status and education level were also taken into consideration. Diet type, saltiness, spiciness and temperature association was critically analyzed. Blood group, family history, smoking habit and alcohol consumption were also recorded. Results. A total of 150 patients with gastric cancer were involved in this study. Male to female ratio was 1.3 : 1. The median ages of male and female were 61 and 52 years, respectively. The tumor distribution by anatomical site was as follows: the lesion was distal in 83 (55 %) patients, proximal in 26 (17 %), involved the body and fundus in 16 (11 %), the entire stomach in 12 (8 %). In 13 (9 %) of cases, lesser curve was the site. The commonest histologic subtype was adenocarcinoma of the intestinal type in 69 patients (46 %). Diffuse type was seen in only 43 (29 %) patients, 14 (9 %) had mixed and in 24 (16 %), the histopathology was unclassifiable. Ulcerative lesion was reported in 57 % of cases. Polypoid or fungating lesions were found in 28 % and infiltrative in 15 %. The commonest endoscopic finding was ulcerative type seen in 57 % of patients. Most of the gastric carcinoma cases (44 %) fell in stage IV disease. Among people with stage IV, only 11 have Her-2 status, negative in 10 cases (15.15 %) and positive in only one patient. The commonest site for metastases was in the liver followed by peritoneum. Conclusions. Despite its low incidence, some epidemiological features of gastric cancer in Iraq mimic those of the high-risk countries. Adenocarcinoma accounts for the highest number of gastric cancers. Most patients are in their 5 and 6 decades of life. The incidence of gastric carcinoma in patients younger than 50 years is higher than in the Western world. Compared to Western literature, our patients were presenting more with intestinal-type adenocarcinoma and less with diffuse type. Most patients had advanced stages of the disease.
рак шлунка; аденокарцинома; Іракська рада з питань раку; кишковий тип за класифікацією Лорена; шлунок
gastric cancer; adenocarcinoma; Iraqi Cancer Board; Lauren intestinal type; stomach
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Roukos DH, Agnantis NJ, Fatouros M, Kappas AM. Gastric cancer: introduction, pathology, epidemiology. Gastric Breast Cancer. 2002;1(1):1-3. Available from: https://www.scirp.org/reference/refe–ren–cespapers?referenceid=1538092.
- Morgan D. The changing epidemiology of gastric cancer. Ameri–can Gastroenterological Association. 2012. Available from: http://www.gastro.org/journals-publications/aga-perspectives/octobernovember-2012/the-changing-epidemiology-of-gastric-cancer.
- Gastric (stomach) cancer. No Stomach for Cancer. 2012. Avai–lable from: http://www.nostomachforcancer.org/gastric-cancer.
- Al Hasnawi SM, Al Mosawi AJ, Khzaie AA, Unan OF, Fadhil HM, Sami S. Cancer in Iraq: distribution by primary tumor site. New Iraqi J Med. 2009;5:5-8. Available from: https://www.researchgate.net/publication/268687758_Cancer_in_Iraq_Distribution_by_primary_tumor_site.
- Iraqi Cancer Board. Results of the Iraqi Cancer Registry 2010. Baghdad: Iraqi Cancer Registry Center, Ministry of Health; 2012. Available from: https://moh.gov.iq/upload/163cancer%20rigistry%202010.pdf.
- Pisters PW, Kelsen DP, Tepper JE. Cancer of the stomach. In: DeVita VT, Hellman S, Rosenberg SA, eds. Cancer: principles & practice of oncology. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2008.
- Alberts SR, Goldberg RM. Gastrointestinal tract cancers. In: Casciato DA, ed. Manual of clinical oncology. 7th ed. Lippincott Williams & Wilkins; 2014.
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, et al. Globocan 2012 v1.0, cancer incidence and mortality worldwide: IARC Cancer Base No. 11. Lyon, France: International Agency for Research on Cancer; 2013. doi: 10.1002/ijc.29210.
- Hussein NR. Helicobacter pylori and gastric cancer in the Middle East: a new enigma? World J Gastroenterol. 2010 Jul 14;16(26):3226-3234. doi: 10.3748/wjg.v16.i26.3226.
- Wu H, Rusiecki JA, Zhu K, Potter J, Devesa SS. Sto–mach carcinoma incidence patterns in the United States by histologic type and anatomic site. Cancer Epidemiol Biomarkers Prev. 2009 Jul;18(7):1945-1952. doi: 10.1158/1055-9965.epi-09-0250.
- Inoue M, Tsugane S. Epidemiology of gastric cancer in Japan. Postgrad Med J. 2005;81:419-424. doi: 10.1136/pgmj.2004.029330.
- Paika DC, Saborioa DV, Oropezaa R, Freemana HP. The epidemiological enigma of gastric cancer rates in the US: was grandmother’s sausage the cause? Int J Epidemiol. 2001;30(1):181-182. doi: 10.1093/ije/30.1.181.
- Forman D, Pisani P. Gastric cancer in Japan — honing treatment, seeking causes. N Engl J Med. 2008;359(5):448-451. doi: 10.1056/nejmp0804354.
- Kabir MA, Barua R, Masud H, Ahmed DS, Karim E, et al. Clinical presentation, histological findings and prevalence of Helicobacter pylori in patients of gastric carcinoma. FMCJ. 2011;6(2):78-81. doi: 10.3329/fmcj.v6i2.9205.
- Asombang AW, Rahman R, Ibdah JA. Gastric cancer in Africa: current management and outcomes. World J Gastroenterol. 2014 Apr 14;20(14):3875-3879. doi: 10.3748/wjg.v20.i14.3875.
- Qurieshi MA, Masoodi MA, Kadla SA, Ahmad SZ, Gangadharan P. Gastric cancer in Kashmir. Asian Pac J Cancer Prev. 2011;12:303-307. Available from: https://pubmed.ncbi.nlm.nih.gov/21517276/.
- Abbasi SY, Taani HE, Saad A, Badheeb A, Addasi A. Advanced gastric cancer in Jordan from 2004 to 2008: a study of epidemiology and outcomes. Gastrointest Cancer Res. 2011;4(4):122-127. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3283110/.
- Halder SK, Bhattacharjee PK, Bhar P, Bhattacharya P, Pachaury A, et al. Demographic and clinico-pathological profile of carcinoma stomach in a tertiary referral centre of Eastern India. Al Ameen J Med Sci. 2012;5(4):398-402. Available from: https://doaj.org/article/a4475e23b5fc4bdeb286a4e8aed57a01.
- Hermiz RS, Hussain AG, Qasim BJ. Immunohistochemi–cal expression of p53 in gastric carcinoma (a clinicopathological study). Iraqi J Med Sci. 2008;6(2):77-89. Available from: https://www.colmed-alnahrain.edu.iq/iraqijms/Iraqi%20JMS%20-%20Volume%206%20(2)%202008/HTML/files/assets/downloads/page0083.pdf.
- Eskandar H, Mohammad SS, Rahim M, Jalal H, Mehrdad A, Rajabi T. Clinical profile of gastric cancer in Khuzestan, southwest of Iran. World J Gastroenterol. 2006 Aug 14;12(30):4832-4835. doi: 10.3748/wjg.v12.i30.4832.
- Misleh JG, Santoro P, Strasser JF, Bennett JJ. Multidisciplinary management of gastric cancer. Surg Oncol Clin N Am. 2013 Apr;22(2):247-264. doi: 10.1016/j.soc.2012.12.013.
- American Cancer Society. Stomach cancer. Revised 2014 May 27. Available from: http://www.cancer.org/cancer/stomachcancer/detailedguide/stomach-cancer-survival-rates.
- Safaee A, Moghimi-Dehkordi B, Fatemi SR, Ghiasi S, Pourhoseingholi MA, Zali MR. Clinicopathological features of gastric cancer: a study based on cancer registry data. IJCP. 2009;2:67-70. Available from: https://brieflands.com/articles/ijcm-80529.
- Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol. 2006 Jan 21;12(3):354-362. doi: 10.3748/wjg.v12.i3.354.
- Van Loon AJ, Goldbohm RA, van den Brandt PA. Socioeconomic status and stomach cancer incidence in men: results from the Netherlands Cohort Study. J Epidemiol Community Health. 1998 Mar;52(3):166-171. doi: 10.1136/jech.52.3.166.
- Chan EE, George TJ. Gastric cancers. In: Abraham J, Gulley J, Allegra C, eds. The Bethesda handbook of clinical oncology. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2014. Available from: https://jasulib.org.kg/wp-content/uploads/2022/10/1.-The-Bethesda-Handbook-of-Clinical-Oncology-PDFDrive-1-1.pdf.
- Kantarjian HM, Wolff RA, Koller CA, eds. The MD Anderson manual of medical oncology. 2nd ed. Texas: McGraw-Hill; 2011. Available from: https://mli.ochsner.org/eBooks/The%20MD%20Anderson%20Manual%20of%20Medical%20Oncology%203e.pdf.
- Wroblewski LE, Peek RM Jr, Wilson KT. Helicobacter pylori and gastric cancer: factors that modulate disease risk. Clin Microbiol Rev. 2010 Oct;23(4):713-739. doi: 10.1128/cmr.00011-10.
- Parsonnet J, Vandersteen D, Goates J, Sibley RK, Pritikin J, Chang Y. Helicobacter pylori infection in intestinal- and diffuse-type gastric adenocarcinomas. J Natl Cancer Inst. 1991 May 1;83(9):640-643. doi: 10.1093/jnci/83.9.640.
- Stomach cancer incidence statistics. Cancer Research UK. 2014 Apr 30. Available from: http://www.cancerresearchuk.org/cancer-info/cancerstats/types/stomach/incidence/uk-stomach-cancer-incidence-statistics.
- Better Health Channel. Stomach cancer — some possible causes. State of Victoria. 2013. Available from: www.betterhealth.vic.gov.au.
- Bani-Hani KE, Yaghan RJ, Heis HA, Shatnawi NJ, Matalka II, et al. Gastric malignancies in Northern Jordan with special emphasis on descriptive epidemiology. World J Gastroenterol. 2004 Aug 1;10(15):2174-2178. doi: 10.3748/wjg.v10.i15.2174.
- Rüschoff J, Hanna W, Bilous M, Hofmann M, Osamura RY, Penault-Llorca F. HER2 testing in gastric cancer: a practical approach. Mod Pathol. 2012;25:637-650. doi: 10.1038/modpathol.2011.198.
- Park DI, Yun JW, Park JH, Oh SJ, Kim HJ, Cho YK, et al. HER-2/neu amplification is an independent prognostic factor in gastric cancer. Dig Dis Sci. 2006;51(8):1371-1379. doi: 10.1007/s10620-005-9057-1.
- Tanner M, Hollmen M, Junttila TT, Kapanen AI, Tommola S, Soini Y, et al. Amplification of HER-2 in gastric carcinoma: association with Topoisomerase IIα gene amplification, intestinal type, poor prognosis and sensitivity to trastuzumab. Ann Oncol. 2005 Feb;16(2):273-278. doi: 10.1093/annonc/mdi064.
- Mehrabani D, Hosseini SV, Rezaianzadeh A, Amini M, Mehrabani G, Tarrahi MJ. Prevalence of stomach cancer in Shiraz, Southern Iran. J Res Med Sci. 2013 Apr;18(4):335-337. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3793381/.
- Alshewered AS, Al-Naqqash MA. Rectal cancer and chemoradiation in Iraq: systematic review and meta-analysis. J Coloproctol. 2019;39(4):309-318. doi: 10.1016/j.jcol.2019.06.003.
- Lazim QJ, Al-Bdaer EK, Mohammed HH, Almirtah DS, Alshewered AS. Diagnosis of Merkel cell carcinoma at chronic venous ulcer: case report. Onkol Radioter. 2020;14(2):1-4. Available from: https://www.researchgate.net/publication/341651463_Diagnosis_of_merkel_cell_carcinoma_at_chronic_venous_ulcer_case_report.
- Alwan AF, Al-Naqqash MA, Al-Nuami HSA, Al-shewe–red AS, Al-Nuami D. Assessment of dose-volume histogram statistics using three-dimensional conformal techniques in breast cancer adjuvant radiotherapy treatment. Precis Radiat Oncol. 2022;6(3):225-233. doi: 10.1002/pro6.1172.
- Al-Rawi SAI, Abouelenein H, Nagdy ME, Khalil MM, Alshewered AS. Assessment of dose gradient index variation during simultaneously integrated boost intensity-modulated radiation therapy for head and neck cancer patients. Precis Radiat Oncol. 2022;6(3):216-224. Available from: https://onlinelibrary.wiley.com/doi/pdf/10.1002/pro6.1166.
- Alashoor MF, Al-Maliki HSK, Al-Khalidy KFA, Alshewe–red AS. Glioblastoma multiform prognosis beyond craniotomy and chemo irradiation. Onkol Radioter. 2022;16(2):38-41. Available from: https://www.researchgate.net/publication/359441916_Glioblastoma_multiform_prognosis_beyond_craniotomy_and_chemo_irradiation.
- Alrubai MAM, Al-Naqqash MA, Alshewered AS. Epidemiological and prognostic single center study of anal carcinoma. J Coloproctol. 2020;40(3):202-208. doi: 10.1016/j.jcol.2020.01.003.
- Alrubai AMM, Al-Jassani HMA, Alsaymaree SMR, Alshe–wered AS. Dermatological sequel of adjuvant breast cancer radiotherapy in Iraqi women. Onkol Radioter. 2020;14(6):1-7. Available from: https://www.researchgate.net/profile/Ahmed-Alshewered/publication/346036773_Dermatological_sequel_of_adjuvant_breast_cancer_radiotherapy_in_Iraqi_women/links/5ff83867299bf140887e0a4f/Dermatological-sequel-of-adjuvant-breast-cancer-radiotherapy-in-Iraqi-women.pdf
- Alshewered A, Kadhim SA. Evaluation of colon cancer incidence rates for the years 2016–2021, Najaf/Iraq: a study of risk assessment. Surg Gastroenterol Oncol. 2024;28:s19-s23. doi: 10.21614/sgo-636.