
Журнал "Гастроэнтерология" Том 59, №3, 2025
Вернуться к номеру
Роль трансректального ультразвукового дослідження в оцінці тяжкості та диференціальній діагностиці запальних захворювань кишечника: порівняльний аналіз при виразковому коліті та хворобі Крона
Авторы: M.V. Stoikevych, T.S. Tarasova, M.V. Titova, O.V. Simonova, O.P. Petishko
Institute of Gastroenterology of NAMSU, Dnipro, Ukraine
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
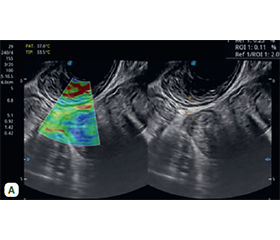
Актуальність. Колоноскопія з біопсією залишається золотим стандартом діагностики запальних захворювань кишечника (ЗЗК). Однак цей метод має низку обмежень, особливо у важких клінічних умовах, тому зростає потреба в менш інвазивних методах візуалізації. Одним із таких методів є трансректальне ультразвукове дослідження (ТРУЗД), яке забезпечує візуалізацію стінки прямої та дистального відділу сигмовидної кишки з високим рівнем деталізації. ТРУЗД дозволяє кількісно оцінити товщину кишкової стінки, стратифікувати її шари, виявити гіперваскуляризацію, характерну для активного запалення, а також інфільтративні й фіброзні зміни. За даними сучасних клінічних досліджень продемонстровано високу чутливість і специфічність цього методу, що робить доцільним більш широке його використання в клінічній практиці. Однак, незважаючи на численні переваги, ТРУЗД у клінічній практиці застосовують недостатньо, хоча воно є перспективним неінвазивним інструментом діагностики й моніторингу пацієнтів із ЗЗК. Мета: проаналізувати можливості й клінічну ефективність трансректального ультразвукового дослідження в діагностиці виразкового коліту (ВК) і хвороби Крона (ХК). Матеріали та методи. ТРУЗД проводили на ультразвуковому сканері експертного класу SonoScape S60 з використанням низькочастотного конвексного датчика 3,5 МГц та ректовагінального конвексного датчика 6 МГц. Використовували трансперинеальний і трансректальний доступи. Результати. Потовщення стінки прямої кишки > 5 мм мали 100 % хворих. Товщина стінки прямої кишки в пацієнтів із ХК була вірогідно нижчою, ніж в осіб із ВК: (5,99 ± 0,42) мм проти (7,12 ± 0,20) мм (р = 0,01). Товщина слизового шару при ВК перевищувала цей показник при ХК в 1,8 раза (p = 0,05), а товщина підслизового шару — в 1,3 (p = 0,01). Товщина м᾽язового шару в пацієнтів із ХК, навпаки, була вірогідно вищою, ніж в осіб із ВК: (1,69 ± 0,21) мм проти (1,17 ± 0,04) мм (p = 0,05). Товщина стінки прямої кишки ((6,80 ± 0,21) мм та (8,15 ± 0,42) мм, р = 0,04) і товщина підслизового шару ((4,14 ± 0,21) мм проти (5,28 ± 0,28) мм, р = 0,008) вірогідно відрізнялися при середньому й тяжкому ступені ВК. Майже у 86,7 % обстежених пацієнтів із тяжким ВК спостерігався 3 ступінь щільності кровотоку у стінці прямої кишки, тоді як при ХК середньої тяжкості 61,5 % пацієнтів мали 1 ступінь. При проведенні еластометрії стінки прямої кишки відмічалася тенденція до збільшення коефіцієнту деформації в пацієнтів із ХК порівняно з особами з ВК. ROC-аналіз дозволив установити високу значущість товщини м’язового шару в диференціальній діагностиці ВК та ХК. Висока діагностична цінність була також отримана щодо товщини підслизового шару при оцінці ступеня тяжкості ВК. Висновки. ТРУЗД є ефективним неінвазивним методом оцінки запальних захворювань кишечника. Допплерівське сканування дозволяє оцінити ступінь васкуляризації стінки прямої кишки, що корелює з клінічною активністю ЗЗК. Еластометрія стінки прямої кишки корисна у визначенні тяжкості запалення. Товщина стінки прямої кишки та підслизового шару має високу прогностичну цінність у виявленні тяжкого ВК. Товщина м’язового шару > 1,3 мм може бути використана як допоміжний критерій у диференціальній діагностиці ВК та ХК.
Background. Colonoscopy with biopsy remains the gold standard for the diagnosis of inflammatory bowel disease (IBD). However, this method has a number of limitations, especially in severe clinical conditions. In this regard, there is a growing need for less invasive imaging methods. One of these methods is transrectal ultrasound (TRUSD), which provides high-resolution imaging of the wall of the rectum and distal sigmoid colon. TRUSD allows for quantitative assessment of the intestinal wall thickness, stratification of its layers, detection of hypervascularisation characteristic of active inflammation, as well as identification of infiltrative and fibrotic changes. The data of modern clinical trials demonstrate the high sensitivity and specificity of this method, which makes it advisable to use TRUSD more widely in clinical practice. Despite its numerous advantages, TRUSD remains an underutilised method in clinical practice, although it is a promising non-invasive tool for the diagnosis and monitoring of patients with IBD. The aim of the study was to analyse the possibilities and clinical effectiveness of transrectal ultrasound in the diagnosis of ulcerative colitis (UC) and Crohn’s disease (CD). Materials and methods. TRUSD was performed on an expert-class ultrasound scanner SonoScape S60 using a 3.5 MHz low-frequency convection transducer and a 6 MHz recto-vaginal convection transducer. Transperineal and transrectal approaches were used. Results. Thickening of the rectal wall > 5 mm was typical for 100 % of patients. The wall thickness was significantly lower in patients with CD compared to those with UC — (5.99 ± 0.42) mm vs. (7.12 ± 0.20) mm, respectively (p = 0.01). The thickness of the mucosal layer in UC was 1.8 times higher than in CD (p = 0.05), and the thickness of the submucosal layer was 1.3 times higher (p = 0.01). On the contrary, the thickness of the muscular layer in patients with CD was significantly higher than in those with UC — (1.69 ± 0.21) mm vs. (1.17 ± 0.04) mm (p = 0.05). The wall thickness ((6.80 ± 0.21) mm vs. (8.15 ± 0.42) mm, p = 0.04) and submucosal layer thickness ((4.14 ± 0.21) mm vs. (5.28 ± 0.28) mm, p = 0.008) significantly differed between moderate and severe UC. Almost 86.7 % of the examined patients with severe UC had grade 3 blood flow density in the rectal wall, whereas in moderate UC, 61.5 % of patients had grade 1. When performing elastometry of the intestinal wall, there was a tendency to increase the strain coefficient in patients with CD compared to UC. The ROC analysis allowed us to establish the high quality of the diagnostic indicator — the thickness of the muscular layer — for the differential diagnosis of UC and CD. High diagnostic value was also obtained for the thickness of the submucosal layer in assessing the severity of UC. Conclusions. TRUSD is an effective non-invasive method for evaluating inflammatory bowel diseases. Doppler scanning allows to assess the degree of vascularisation of the intestinal wall, which correlates with the clinical activity of IBD. Intestinal wall elastometry is useful in determining the severity of inflammation. The thickness of the intestinal wall and submucosa have a high prognostic value in detecting severe UC. A muscular layer thickness of 1.3 mm can be used as an auxiliary criterion for the differential diagnosis between UC and CD.
трансректальне ультразвукове дослідження; виразковий коліт; хвороба Крона
transrectal ultrasound examination; ulcerative colitis; Crohn’s disease
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Feuerstein JD, Cheifetz AS. Crohn Disease: Epidemiology, Diag–nosis and Management. Mayo Clin Proc. 2017;92(7):1088-1103. doi: 10.1016/j.mayocp.2017.04.010.
- Windsor JW, Kaplan GG. Evolving Epidemiology of IBD. Curr Gastroenterol Rep. 2019;21(8):40. doi: 10.1007/s11894-019-0705-6.
- Click B, Cross R, Regueiro M, Keefer L. The IBD Clinic of Tomorrow: Holistic, Patient-Centric, and Value-based Care. Clin Gastroenterol Hepatol. 2025;23(3):419-427.e3. doi: 10.1016/j.cgh.2024.04.042.
- Singh A, Bhardwaj A, Sharma R, Midha V, Sood A. Developing IBD counsellors in low- and middle-income countries: bridging gaps in patient care. EClinicalMedicine. 2025;83:103218. doi: 10.1016/j.eclinm.2025.103218.
- Tavakoli P, Vollmer-Conna U, Hadzi-Pavlovic D, Grimm MC. A Review of Inflammatory Bowel Disease: A Model of Microbial, Immune and Neuropsychological Integration. Public Health Rev. 2021;42:1603990. doi: 10.3389/phrs.2021.1603990.
- Maaser C, et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial Diagnosis, Monitoring of Known IBD, Detection of Complications. J Crohns Colitis. 2019;13(2):144-164. doi: 10.1093/ecco-jcc/jjy113.
- Christian M, et al. Ultrasonography in inflammatory bo–wel disease — So far we are? United European Gastroenterol J. 2022;10(2):225-232. doi: 10.1002/ueg2.12196.
- Dolinger MT, et al. Current and Novel Uses of Intestinal Ultrasound in Inflammatory Bowel Disease. Gastroenterol Hepatol (NY). 2023;19(8):447-457.
- Noor NM, Sousa P, Paul S, Roblin X. Early Diagnosis, Early Stratification, and Early Intervention to Deliver Precision Medicine in IBD. Inflamm Bowel Dis. 2022;28(8):1254-1264. doi: 10.1093/ibd/izab228.
- Novak KL, Wilson SR. The role of ultrasound in the evaluation of inflammatory bowel disease. Semin Roentgenol. 2013;48(3):224-33. doi: 10.1053/j.ro.2013.03.003.
- Shaban N, et al. Imaging in inflammatory bowel disease: current and future perspectives. Frontline Gastroenterol. 2022;13:e28-e34. doi: 10.1136/flgastro-2022-102117.
- Krugliak Cleveland N, St-Pierre J, Kellar A, Rubin DT. Clinical Application of Intestinal Ultrasound in Inflammatory Bowel Disease. Curr Gastroenterol Rep. 2024;26(2):31-40. doi: 10.1007/s11894-024-00915-x.
- Pal P, et al. Transperineal ultrasound: Role in inflammatory bowel disease management. World J Gastroenterol. 2025;31(33):109811. doi: 10.3748/wjg.v31.i33.109811.
- Yan B, et al. Reliability of EUS indices to detect inflammation in ulcerative colitis. Gastrointest Endosc. 2017;86(6):1079-1087. doi: 10.1016/j.gie.2017.07.035.
- Yan BM, et al. Reliability of the Endoscopic Ultrasound Ulce–rative Colitis (EUS-UC) score for assessment of inflammation in patients with ulcerative colitis. Endosc Int Open. 2021;9(7):E1116-E1122. doi: 10.1055/a-1481-8032.
- Statie RC, Florescu DN, Gheonea DI, Ungureanu BS, Iordache S, et al. The Use of Endoscopic Ultrasonography in Inflammatory Bowel Disease: A Review of the Literature. Diagnostics (Basel). 2023;13(3):568. doi: 10.3390/diagnostics13030568.
- Rogler G. No Need to Scope? Monitoring of Treatment Response in IBD Patients by Transabdominal Ultrasound. J Crohns Colitis. 2022;16(4):521-522. doi: 10.1093/ecco-jcc/jjab220.
- Rustemovic N, et al. A pilot study of transrectal endoscopic ultrasound elastography in inflammatory bowel disease. BMC Gastroenterol. 2011;11:113. doi: 10.1186/1471-230x-11-113.
- Bapaye J, Chandan S, Kochhar GS. Role of Endosco–pic Ultrasound in the Diagnosis and Management of Complications of Inflammatory Bowel Disease. Gastrointest Endosc Clin N Am. 2025;35(1):235-253. doi: 10.1016/j.giec.2024.07.005.
- Innocenti T, Rocco C, Balena E, Petrucci G, Lynch EN, et al. The use of International Bowel Ultrasound Segmental Activity Score (IBUS-SAS) in patients with ulcerative colitis: applicabili–ty and comparison with other ultrasound scores. J Crohns Colitis. 2025;19(5):jjaf050. doi: 10.1093/ecco-jcc/jjaf050.